Walker S H, Gokhale L
Department of Obstetrics and Gynaecology, Royal Gwent Hospital, Aneurin Bevan University Health Board, Newport, UK.
Gynecol Surg. 2018;15(1):2. doi: 10.1186/s10397-018-1036-6. Epub 2018 Jan 15.
The purpose of this study is to evaluate current practice amongst gynaecologists across the UK, regarding safety aspects of inpatient hysteroscopy under anaesthesia, specifically in relation to entry and specimen retrieval.A survey was created using survey monkey. The first round was circulated to all registrar trainees and consultant gynaecologists across Wales. Following a good response, the survey was then circulated to all members of the British Society of Gynaecological Endoscopy (BSGE).
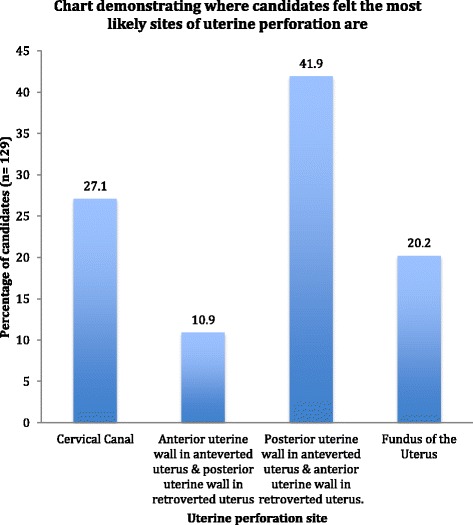
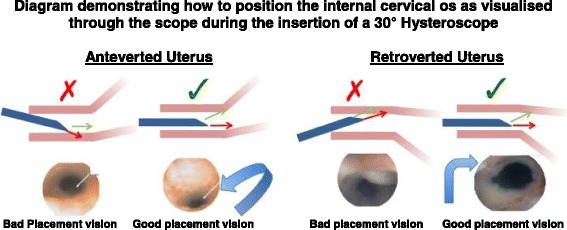
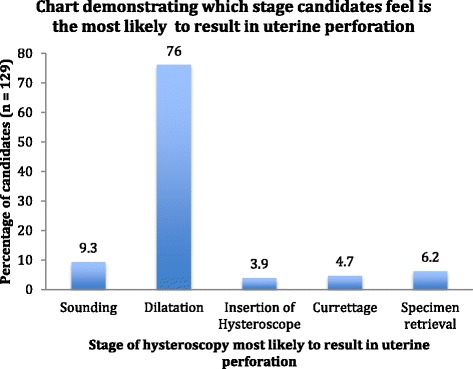
There were 212 responses including, 140 consultants, 36 senior registrars, 17 junior registrars and 18 clinical nurse specialists. In total, 136 out of 212 (64.7%) always perform a vaginal examination prior to hysteroscopy. 10.4% always sound the uterus, and 5.2% always dilate the uterus prior to insertion of the hysteroscope. Twenty-three consultants, six senior registrars, three junior registrars and one clinical nurse specialist knew how to position the internal cervical os as visualised through the scope when using a 30° hysteroscope. 35.8% of candidates always perform a post-procedure cavity check, and 9% use suction to flush the cavity to aid vision during the post-procedure cavity check. The majority (76%) predicted dilatation as the stage most likely to cause uterine perforation and predicted the most likely site for perforation as the posterior uterine wall in the anteverted uterus and the anterior uterine wall in the retroverted uterus.
This study highlights varied practice across the UK regarding safety aspects of hysteroscopy, in relation to entry and specimen retrieval. There is a need for increased awareness of the risks of hysteroscopy and paramount precautions that should be performed routinely as part of their practice. Standardised guidelines may be a beneficial tool to help bring about this change in practice, leading to a reduction in uterine perforation rates.
本研究旨在评估英国妇科医生在麻醉下住院宫腔镜检查安全方面的当前做法,特别是在进入和标本获取方面。使用SurveyMonkey创建了一项调查。第一轮调查发送给了威尔士所有的住院医师培训学员和妇科顾问医生。在收到良好反馈后,该调查随后发送给了英国妇科内镜学会(BSGE)的所有成员。
共收到212份回复,其中包括140名顾问医生、36名高级住院医师、17名初级住院医师和18名临床护士专家。在212名受访者中,共有136人(64.7%)在宫腔镜检查前总是进行阴道检查。10.4%的人总是探测子宫,5.2%的人在插入宫腔镜前总是扩张子宫。23名顾问医生、6名高级住院医师、3名初级住院医师和1名临床护士专家知道在使用30°宫腔镜时如何通过镜下观察定位子宫颈内口。35.8%的受访者在术后总是进行宫腔检查,9%的人在术后宫腔检查时使用吸引器冲洗宫腔以辅助观察。大多数人(76%)预测扩张是最有可能导致子宫穿孔的阶段,并预测前位子宫穿孔最可能的部位是子宫后壁,后位子宫是子宫前壁。
本研究强调了英国在宫腔镜检查安全方面,在进入和标本获取方面存在不同的做法。有必要提高对宫腔镜检查风险的认识以及作为其常规操作一部分应采取的首要预防措施。标准化指南可能是有助于在实践中带来这种改变的有益工具,从而降低子宫穿孔率。