Lagrou Daphne, Zachariah Rony, Bissell Karen, Van Overloop Catherine, Nasim Masood, Wagma Hamsaya Nikyar, Kakar Shafiqa, Caluwaerts Séverine, De Plecker Eva, Fricke Renzo, Van den Bergh Rafael
1Medical department, Mother and Child Health Unit, Brussels Operational Centre, Médecins Sans Frontières, Rue de l'Arbre Bénit 46, 1050 Brussels, Belgium.
2Medical department (Operational Research), Operational Centre Brussels, Médecins Sans Frontières, Luxembourg City, Luxembourg.
Confl Health. 2018 Jan 22;12:2. doi: 10.1186/s13031-018-0137-1. eCollection 2018.
Provision of Emergency Obstetric and Neonatal Care (EmONC) reduces maternal mortality and should include three components: Basic Emergency Obstetric and Neonatal Care (BEmONC) offered at primary care level, Comprehensive EmONC (CEmONC) at secondary level and a good referral system in-between. In a conflict-affected province of Afghanistan (Khost), we assessed the performance of an Médecins Sans Frontières (MSF) run CEmONC hospital without a primary care and referral system. Performance was assessed in terms of hospital utilisation for obstetric emergencies and quality of obstetric care.
A cross-sectional study using routine programme data (2013-2014).
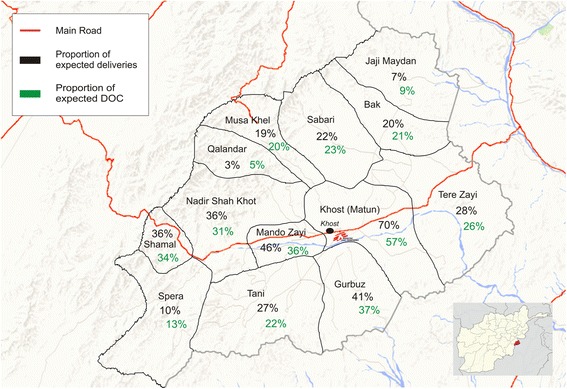
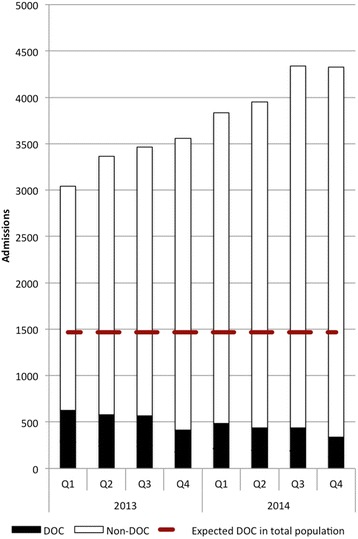
Of 29,876 admissions, 99% were self-referred, 0.4% referred by traditional birth attendants and 0.3% by health facilities. Geographic origins involved clustering around the hospital vicinity and the provincial road axis. While there was a steady increase in hospital caseload, the number and proportion of women with Direct Obstetric Complications (DOC) progressively dropped from 21% to 8% over 2 years. Admissions for normal deliveries continuously increased. In-hospital maternal deaths were 0.03%, neonatal deaths 1% and DOC case-fatality rate 0.2% (all within acceptable limits).
Despite a high and ever increasing caseload, good quality Comprehensive EmONC could be offered in a conflict-affected setting in rural Afghanistan. However, the primary emergency role of the hospital is challenged by diversion of resources to normal deliveries that should happen at primary level. Strengthening Basic EmONC facilities and establishing an efficient referral system are essential to improve access for emergency cases and increase the potential impact on maternal mortality.
提供紧急产科和新生儿护理(EmONC)可降低孕产妇死亡率,且应包括三个组成部分:基层医疗提供的基本紧急产科和新生儿护理(BEmONC)、二级医疗提供的综合EmONC(CEmONC)以及两者之间良好的转诊系统。在阿富汗一个受冲突影响的省份(霍斯特省),我们评估了无基层医疗和转诊系统的无国界医生组织(MSF)运营的CEmONC医院的绩效。从产科急诊的医院利用率和产科护理质量方面对绩效进行了评估。
采用常规项目数据进行横断面研究(2013 - 2014年)。
在29876例入院病例中,99%是自行转诊,0.4%由传统助产士转诊,0.3%由医疗机构转诊。地理来源集中在医院附近和省级道路沿线。虽然医院病例数量稳步增加,但直接产科并发症(DOC)女性的数量和比例在两年内从21%逐渐降至8%。正常分娩的入院人数持续增加。院内孕产妇死亡率为0.03%,新生儿死亡率为1%,DOC病死率为0.2%(均在可接受范围内)。
尽管病例数量居高不下且不断增加,但在阿富汗农村受冲突影响地区仍可提供高质量的综合EmONC。然而,该医院的主要急诊作用受到资源转向正常分娩(正常分娩应在基层进行)的挑战。加强基本EmONC设施并建立高效的转诊系统对于改善急诊病例的就医机会以及增强对孕产妇死亡率的潜在影响至关重要。