Kortman H G, Boukrab I, Bloemsma G, Peluso J P, Sluzewski M, van der Pol B, Beute G N, Majoie C B, van Rooij W J
Department of Radiology, St. Elisabeth Hospital, Tilburg, The Netherlands.
Department of Neurosurgery, St. Elisabeth Hospital, Tilburg, The Netherlands.
J Cerebrovasc Endovasc Neurosurg. 2017 Dec;19(4):284-290. doi: 10.7461/jcen.2017.19.4.284. Epub 2017 Dec 31.
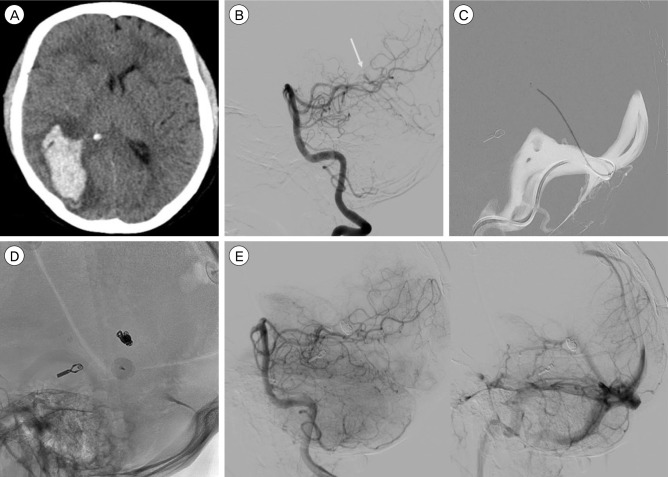
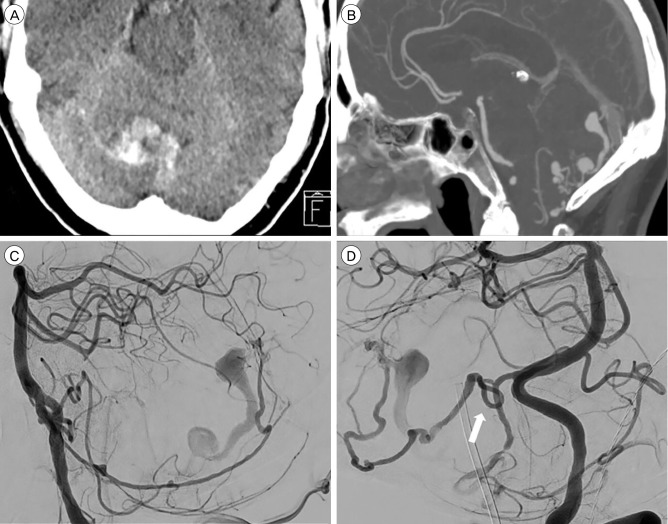
Tentorial dural arteriovenous fistulas usually drain into cortical veins and often present with hemorrhage. Treatment goal is occlusion of the draining vein, either by surgery or endovascular techniques. We present the multimodality treatment results of 12 patients with tentorial dural arteriovenous fistulas.
Between January 2007 and January 2017, 12 consecutive patients with tentorial dural arteriovenous fistulas were treated. There were 11 men and 1 woman with a mean age of 62 years (range 44-85). Clinical presentation was hemorrhage in 8 (67%), pulsatile tinnitus in 2 (17%) and an incidental finding in 2 (17%). The fistula location was at the tentorium cerebelli in 5 (42%), the torcula Herophilii in 4 (33%) and petroclival in 3 (25%).
In 11 patients, arterial embolization with Onyx or PHIL was the primary treatment. Complete obliteration was achieved in one session in 5 (45%) and in 2 sessions in 4 (36%). In 2 patients additional surgery was needed. Primary surgery was performed in 1 patient followed by endovascular coil occlusion via the venous route. One patient with exclusive pial feeders from the posterior inferior cerebellar artery had a clinically silent P3 occlusion during trans arterial embolization. Finally, all 12 fistula were completely occluded, confirmed with angiography after 8-12 weeks. There were no permanent procedural complications.
Patients with tentorial dural arteriovenous fistulas were effectively and safely cured with a strategy of endovascular treatment with various techniques and surgery. Surgical and endovascular techniques are complementary in the treatment of these challenging vascular disorders.
小脑幕硬脑膜动静脉瘘通常引流至皮质静脉,常表现为出血。治疗目标是通过手术或血管内技术闭塞引流静脉。我们展示了12例小脑幕硬脑膜动静脉瘘患者的多模式治疗结果。
2007年1月至2017年1月,连续治疗12例小脑幕硬脑膜动静脉瘘患者。其中男性11例,女性1例,平均年龄62岁(范围44 - 85岁)。临床表现为出血8例(67%),搏动性耳鸣2例(17%),偶然发现2例(17%)。瘘管位于小脑幕5例(42%),窦汇4例(33%),岩斜区3例(25%)。
11例患者以Onyx或PHIL进行动脉栓塞作为主要治疗方法。5例(45%)在一次治疗中实现完全闭塞,4例(36%)在两次治疗中实现完全闭塞。2例患者需要额外手术。1例患者先行手术,随后通过静脉途径进行血管内弹簧圈闭塞。1例由小脑后下动脉单独软膜供血的患者在经动脉栓塞期间出现临床上无症状的P3闭塞。最后,所有12例瘘管均完全闭塞,8 - 12周后经血管造影证实。无永久性手术并发症。
采用多种技术的血管内治疗策略联合手术,可有效、安全地治愈小脑幕硬脑膜动静脉瘘患者。手术和血管内技术在治疗这些具有挑战性的血管疾病中具有互补性。