Kim Claire, Wright Frances C, Look Hong Nicole J, Groot Gary, Helyer Lucy, Meiers Pamela, Quan May Lynn, Urquhart Robin, Warburton Rebecca, Gagliardi Anna R
Department of Clinical Decision Making & Health Care, University Health Network, Toronto, Ontario, Canada.
Department of Surgery, Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada.
PLoS One. 2018 Feb 5;13(2):e0192097. doi: 10.1371/journal.pone.0192097. eCollection 2018.
Active surveillance (AS) represents a fundamental shift in managing select cancer patients that initiates treatment only upon disease progression to avoid overtreatment. Given uncertain outcomes, patient engagement could support decision-making about AS. Little is known about how to optimize patient engagement for AS decision-making. This scoping review aimed to characterize research on patient and provider communication about AS, and associated determinants and outcomes.
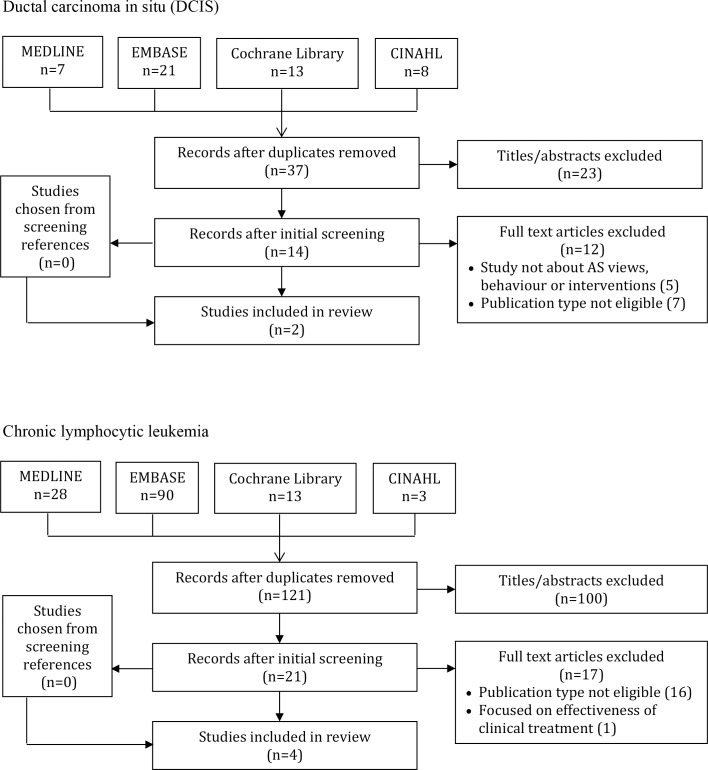
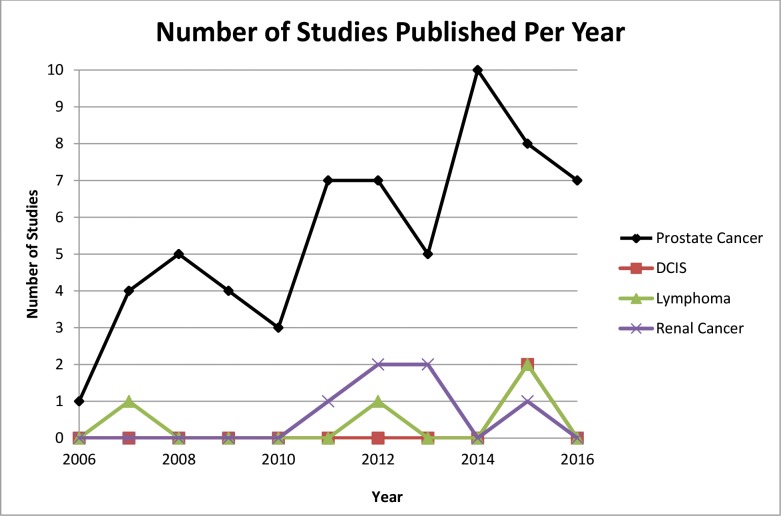
MEDLINE, EMBASE, CINAHL, and The Cochrane Library were searched from 2006 to October 2016. English language studies that evaluated cancer patient or provider AS views, experiences or behavioural interventions were eligible. Screening and data extraction were done in duplicate. Summary statistics were used to describe study characteristics and findings.
A total of 2,078 studies were identified, 1,587 were unique, and 1,243 were excluded based on titles/abstracts. Among 344 full-text articles, 73 studies were eligible: 2 ductal carcinoma in situ (DCIS), 4 chronic lymphocytic leukemia (CLL), 6 renal cell carcinoma (RCC) and 61 prostate cancer. The most influential determinant of initiating AS was physician recommendation. Others included higher socioeconomic status, smaller tumor size, comorbid disease, older age, and preference to avoid adverse treatment effects. AS patients desired more information about AS and reassurance about future treatment options, involvement in decision-making and assessment of illness uncertainty and supportive care needs during follow-up. Only three studies of prostate cancer evaluated interventions to improve AS communication or experience.
This study revealed a paucity of research on AS communication for DCIS, RCC and CLL, but generated insight on how to optimize AS discussions in the context of routine care or clinical trials from research on AS for prostate cancer. Further research is needed on AS for patients with DCIS, RCC and CLL, and to evaluate interventions aimed at patients and/or providers to improve AS communication, experience and associated outcomes.
主动监测(AS)代表了对特定癌症患者管理方式的根本转变,即仅在疾病进展时才开始治疗以避免过度治疗。鉴于结果不确定,患者参与有助于支持关于AS的决策。对于如何优化患者参与AS决策,人们知之甚少。本综述旨在描述关于患者与医护人员就AS进行沟通以及相关决定因素和结果的研究。
检索了2006年至2016年10月期间的MEDLINE、EMBASE、CINAHL和Cochrane图书馆。纳入评估癌症患者或医护人员对AS的看法、经历或行为干预的英文研究。筛选和数据提取由两人独立进行。使用汇总统计数据描述研究特征和结果。
共识别出2078项研究,其中1587项为独特研究,根据标题/摘要排除了1243项。在344篇全文文章中,73项研究符合要求:2项导管原位癌(DCIS)、4项慢性淋巴细胞白血病(CLL)、6项肾细胞癌(RCC)和61项前列腺癌。启动AS的最具影响力的决定因素是医生的建议。其他因素包括较高的社会经济地位、较小的肿瘤大小、合并疾病、年龄较大以及偏好避免不良治疗效果。AS患者希望获得更多关于AS的信息以及对未来治疗选择的安心,希望参与决策,并在随访期间评估疾病不确定性和支持性护理需求。仅有三项前列腺癌研究评估了改善AS沟通或体验的干预措施。
本研究揭示了关于DCIS、RCC和CLL的AS沟通研究匮乏,但从前列腺癌的AS研究中获得了关于如何在常规护理或临床试验背景下优化AS讨论的见解。需要对DCIS、RCC和CLL患者的AS进行进一步研究,并评估针对患者和/或医护人员的干预措施,以改善AS沟通、体验和相关结果。