Chok Lionel, Bachli Esther B, Steiger Peter, Bettex Dominique, Cottini Silvia R, Keller Emanuela, Maggiorini Marco, Schuepbach Reto A
Institute of Intensive Care Medicine, University Hospital Zurich, University Zurich, Raemistrasse 100, CH-8091, Zurich, Switzerland.
Department of Internal Medicine, Hospital Uster, Brunnenstrasse 42, CH-8610, Uster, Zurich, Switzerland.
BMC Health Serv Res. 2018 Feb 5;18(1):84. doi: 10.1186/s12913-018-2869-4.
In 2013 the Swiss Diagnosis Related Groups ((Swiss)-DRG) was implemented in Intensive Care Units (ICU). Its impact on hospitalizations has not yet been examined. We compared the number of ICU admissions, according to clinical severity and referring institution, and screened whether implementation of Swiss-DRG affected admission policy, ICU length-of-stay (ICU-LOS) or ICU mortality.
Retrospective, single centre, cohort study conducted at the University Hospital Zurich, Switzerland between January 2009 and end of September 2013. Demographic and clinical data was retrieved from a quality assurance database.
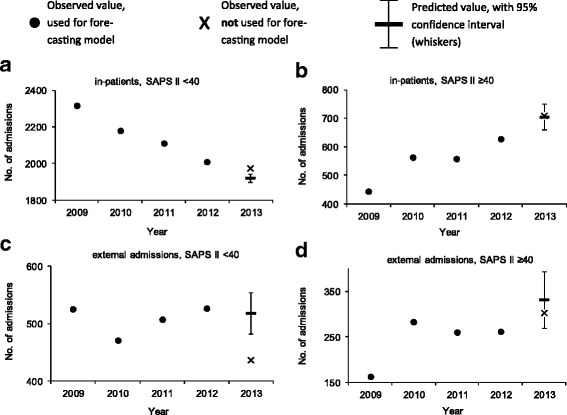
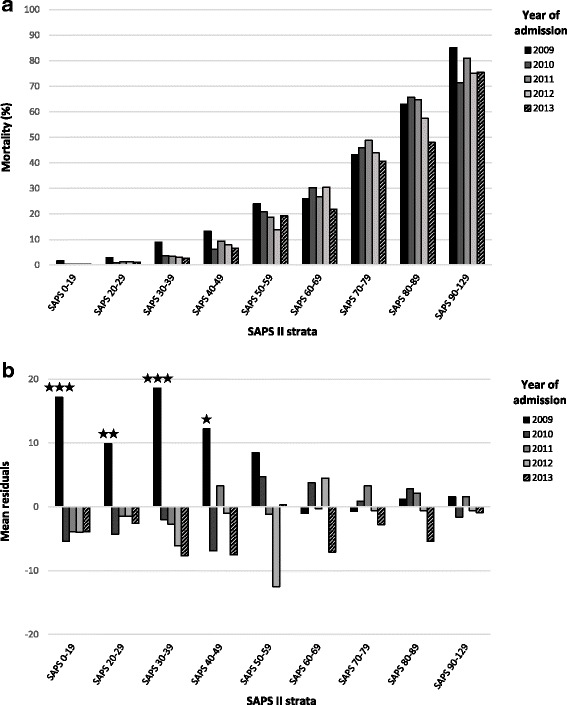
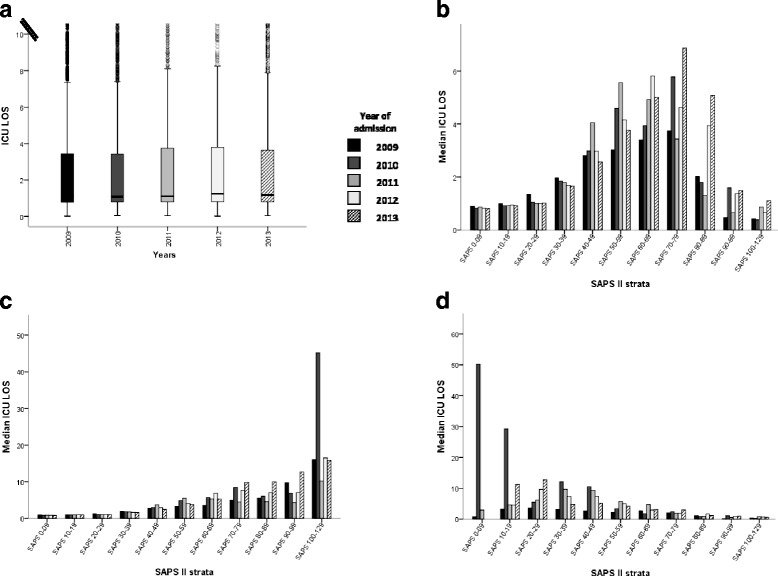
Admissions (n = 17,231) before the introduction of Swiss-DRG were used to model expected admissions after DRG, and then compared to the observed admissions. Forecasting matched observations in patients with a high clinical severity admitted from internal units and external hospitals (admitted / predicted: 709 / 703, [95% Confidence Interval (CI), 658-748] and 302 / 332, [95% CI, 269-365] respectively). In patients with low severity of disease, in-house admissions became more frequent than expected and external admission were less frequent (admitted / predicted: 1972 / 1910, [95% CI, 1898-1940] and 436 / 518, [95% CI, 482-554] respectively). Various mechanisms related to Swiss-DRG may have led to these changes. DRG could not be linked to significant changes in regard to ICU-LOS and ICU mortality.
DRG introduction had not affected ICU admissions policy, except for an increase of in-house patients with a low clinical severity of disease. DRG had neither affected ICU mortality nor ICU-LOS.
2013年,瑞士诊断相关分组((Swiss)-DRG)在重症监护病房(ICU)实施。其对住院治疗的影响尚未得到研究。我们根据临床严重程度和转诊机构比较了ICU入院人数,并筛查了瑞士诊断相关分组的实施是否影响入院政策、ICU住院时间(ICU-LOS)或ICU死亡率。
在瑞士苏黎世大学医院于2009年1月至2013年9月底进行了一项回顾性、单中心队列研究。人口统计学和临床数据从质量保证数据库中获取。
引入瑞士诊断相关分组之前的入院患者(n = 17231)用于模拟诊断相关分组实施后的预期入院人数,然后与观察到的入院人数进行比较。预测结果与从内部科室和外部医院入院的临床严重程度较高的患者的观察结果相符(分别为709 / 703,[95%置信区间(CI),658 - 748]和302 / 332,[95% CI,269 - 365])。在疾病严重程度较低的患者中,内部入院比预期更频繁,外部入院则比预期更不频繁(分别为1972 / 1910,[95% CI,1898 - 1940]和436 / 518,[95% CI,482 - 554])。与瑞士诊断相关分组相关的各种机制可能导致了这些变化。诊断相关分组与ICU住院时间和ICU死亡率的显著变化无关。
除了临床疾病严重程度较低的内部患者入院人数增加外,诊断相关分组的引入并未影响ICU入院政策。诊断相关分组既未影响ICU死亡率,也未影响ICU住院时间。