Bertot Luis C, Jeffrey Gary P, Wallace Michael, MacQuillan Gerry, Garas George, Ching Helena L, Adams Leon A
School of Medicine and Pharmacology University of Western Australia Nedlands Western Australia Australia.
Department of Hepatology Sir Charles Gairdner Hospital Nedlands Western Australia Australia.
Hepatol Commun. 2017 Feb 27;1(1):53-60. doi: 10.1002/hep4.1018. eCollection 2017 Feb.
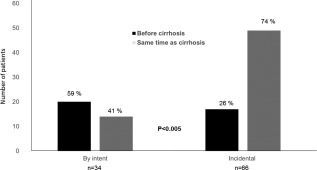
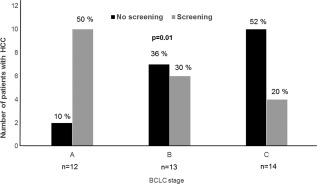
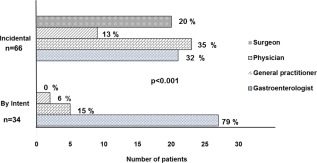
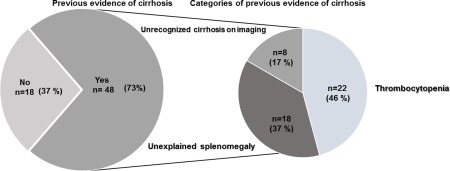
Determination of cirrhosis in nonalcoholic fatty liver disease (NAFLD) is important as it alters prognosis and management. We aimed to examine whether cirrhosis was diagnosed incidentally or intentionally in patients with NAFLD. We reviewed 100 patients with NAFLD cirrhosis to determine mode of cirrhosis diagnosis (incidental or by intent), severity of liver disease at diagnosis, diagnostician, and previous clinical imaging or laboratory evidence of unrecognized cirrhosis. The majority (66/100) of patients with NAFLD cirrhosis were diagnosed incidentally, with the majority of these (74%) diagnosed with NAFLD simultaneously. Those with incidental cirrhosis diagnoses had more deranged platelet and international normalized ratio levels ( < 0.05) and were more likely to have concomitant hepatocellular carcinoma (HCC) (12% versus 0%, < 0.05). Incidental cirrhosis was diagnosed following imaging (32%) or liver tests (26%) performed for reasons unrelated to liver disease, following unexpected endoscopic finding of varices (21%) or an unexpected surgical finding (14%). Diagnoses by intent were predominantly made by gastroenterologists/hepatologists, whereas general practitioners, surgeons, and physicians tended to diagnose cirrhosis incidentally ( < 0.001). The majority of patients diagnosed incidentally (n = 48/66, 73%) had previous thrombocytopenia, splenomegaly, or high noninvasive fibrosis scores. Following diagnosis, patients diagnosed incidentally were less likely to undergo HCC screening. : The majority of patients with NAFLD cirrhosis are diagnosed incidentally. These patients are more likely to have advanced liver disease and HCC. Increased awareness of screening for cirrhosis is needed in patients with NAFLD. (Hepatology Communications 2017;1:53-60).
非酒精性脂肪性肝病(NAFLD)中肝硬化的判定很重要,因为它会改变预后和治疗方案。我们旨在研究NAFLD患者的肝硬化是偶然诊断还是有意诊断的。我们回顾了100例NAFLD肝硬化患者,以确定肝硬化的诊断方式(偶然或有意)、诊断时的肝病严重程度、诊断医生以及既往未被识别的肝硬化的临床影像或实验室证据。大多数(66/100)NAFLD肝硬化患者是偶然诊断的,其中大多数(74%)同时被诊断为NAFLD。那些偶然诊断为肝硬化的患者血小板和国际标准化比值水平更紊乱(P<0.05),并且更有可能合并肝细胞癌(HCC)(12%对0%,P<0.05)。偶然肝硬化是在因与肝病无关的原因进行影像检查(32%)或肝功能检查(26%)后、意外内镜发现静脉曲张(21%)或意外手术发现(14%)后诊断的。有意诊断主要由胃肠病学家/肝病学家做出,而全科医生、外科医生和内科医生倾向于偶然诊断肝硬化(P<0.001)。大多数偶然诊断的患者(n = 48/66,73%)既往有血小板减少、脾肿大或高非侵入性纤维化评分。诊断后,偶然诊断的患者接受HCC筛查的可能性较小。结论:大多数NAFLD肝硬化患者是偶然诊断的。这些患者更有可能患有晚期肝病和HCC。NAFLD患者需要提高对肝硬化筛查的认识。(《肝病通讯》2017年;1:53 - 60)