Jung Su-Young, Kwon Jaeyeol, Park Seohyun, Jhee Jong Hyun, Yun Hae-Ryong, Kim HyoungNae, Kee Youn Kyung, Yoon Chang-Yun, Chang Tae-Ik, Kang Ea Wha, Park Jung Tak, Yoo Tae-Hyun, Kang Shin-Wook, Han Seung Hyeok
Department of Internal Medicine, College of Medicine, Institute of Kidney Disease Research, Yonsei University, Seoul, Korea.
Department of Internal Medicine, NHIS Medical Center, Ilsan Hospital, Ilsan, Korea.
PLoS One. 2018 Feb 7;13(2):e0191290. doi: 10.1371/journal.pone.0191290. eCollection 2018.
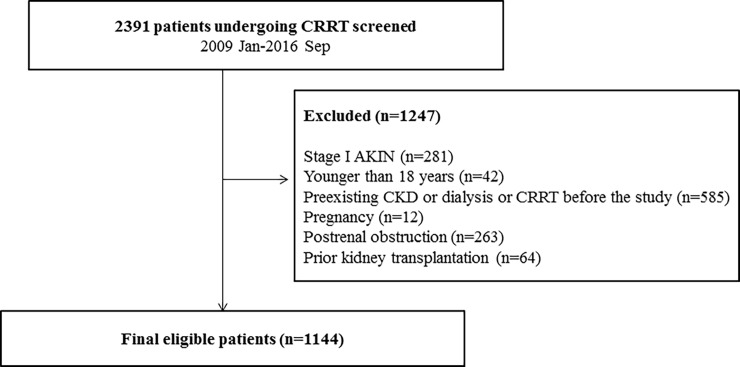
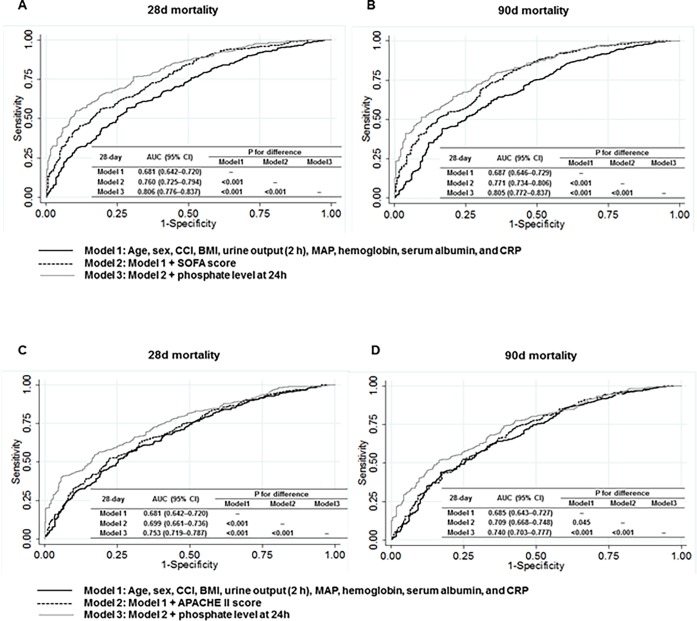
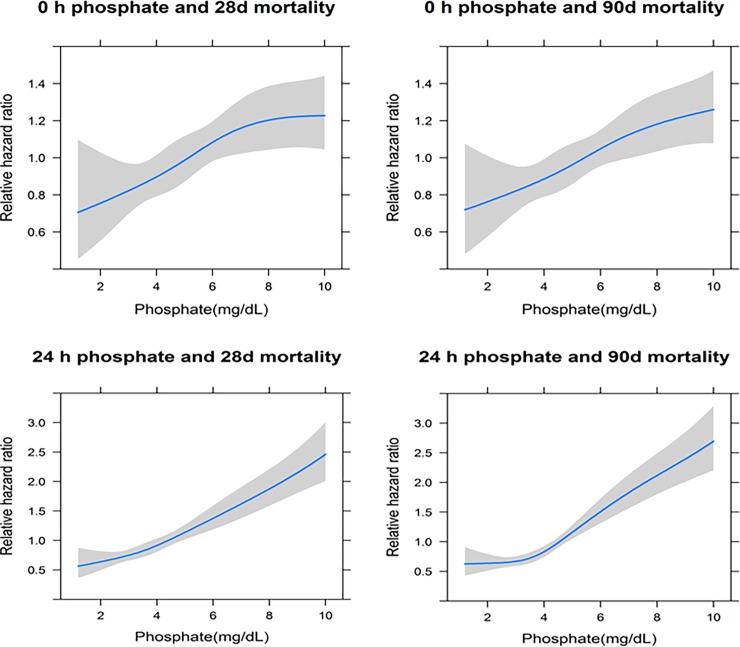
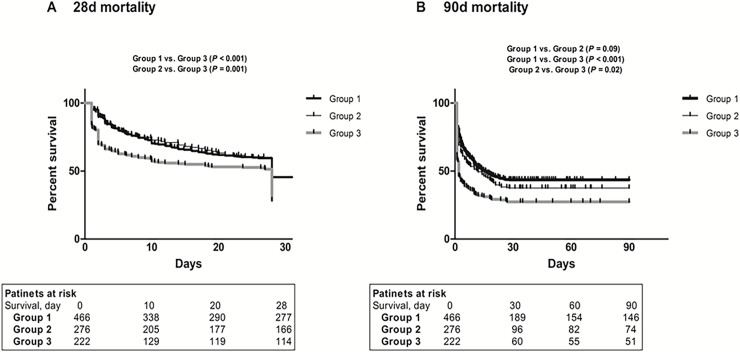
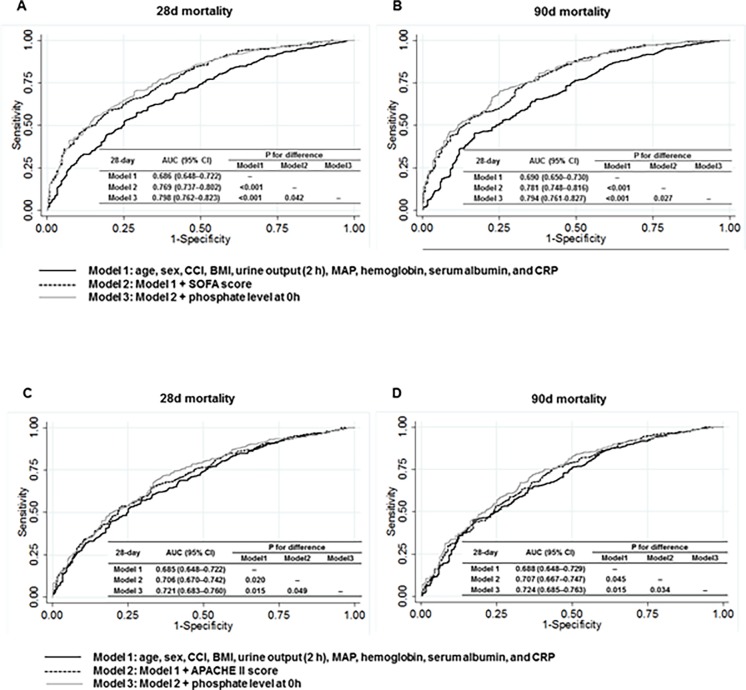
Hyperphosphatemia is associated with mortality in patients with chronic kidney disease, and is common in critically ill patients with acute kidney injury (AKI); however, its clinical implication in these patients is unknown. We conducted an observational study in 1144 patients (mean age, 63.2 years; male, 705 [61.6%]) with AKI who received continuous renal replacement therapy (CRRT) between January 2009 and September 2016. Phosphate levels were measured before (0 h) and 24 h after CRRT initiation. We assessed disease severity using various clinical parameters. Phosphate at 0 h positively correlated with the Acute Physiology and Chronic Health Evaluation II (APACHE II; P < 0.001) and Sequential Organ Failure Assessment (SOFA; P < 0.001) scores, and inversely with mean arterial pressure (MAP; P = 0.02) and urine output (UO; P = 0.01). In a fully adjusted linear regression analysis for age, sex, Charlson comorbidity index (CCI), MAP, and estimated glomerular filtration rate (eGFR), higher 0 h phosphate level was significantly associated with high APACHE II (P < 0.001) and SOFA (P = 0.04) scores, suggesting that phosphate represents disease severity. A multivariable Cox model also showed that hyperphosphatemia was significantly associated with increased 28-day (HR 1.05, 95% CI 1.02-1.08, P = 0.001) and 90-day (HR 1.05, 95% CI 1.02-1.08, P = 0.001) mortality. Furthermore, patients with increased phosphate level during 24 h were at higher risk of death than those with stable or decreased phosphate levels. Finally, c-statistics significantly increased when phosphate was added to a model that included age, sex, CCI, body mass index, eGFR, MAP, hemoglobin, serum albumin, C-reactive protein, and APACHE II score. This study shows that phosphate is a potential biomarker that can reflect disease severity and predict mortality in critically ill patients receiving CRRT.
高磷血症与慢性肾脏病患者的死亡率相关,在急性肾损伤(AKI)的危重症患者中也很常见;然而,其在这些患者中的临床意义尚不清楚。我们对2009年1月至2016年9月期间接受持续肾脏替代治疗(CRRT)的1144例AKI患者(平均年龄63.2岁;男性705例[61.6%])进行了一项观察性研究。在CRRT开始前(0小时)和开始后24小时测量血磷水平。我们使用各种临床参数评估疾病严重程度。0小时时的血磷与急性生理与慢性健康状况评分系统II(APACHE II;P<0.001)和序贯器官衰竭评估(SOFA;P<0.001)评分呈正相关,与平均动脉压(MAP;P=0.02)和尿量(UO;P=0.01)呈负相关。在对年龄、性别、Charlson合并症指数(CCI)、MAP和估计肾小球滤过率(eGFR)进行完全校正的线性回归分析中,较高的0小时血磷水平与高APACHE II(P<0.001)和SOFA(P=0.04)评分显著相关,表明血磷代表疾病严重程度。多变量Cox模型还显示,高磷血症与28天(HR 1.05,95%CI 1.02-1.08,P=0.001)和90天(HR 1.05,95%CI 1.02-1.08,P=0.001)死亡率增加显著相关。此外,血磷水平在24小时内升高的患者比血磷水平稳定或降低的患者死亡风险更高。最后,当将血磷添加到包含年龄、性别、CCI、体重指数、eGFR、MAP、血红蛋白、血清白蛋白、C反应蛋白和APACHE II评分的模型中时,c统计量显著增加。这项研究表明,血磷是一种潜在的生物标志物,可以反映接受CRRT的危重症患者的疾病严重程度并预测死亡率。