van den Boorn H G, Engelhardt E G, van Kleef J, Sprangers M A G, van Oijen M G H, Abu-Hanna A, Zwinderman A H, Coupé V M H, van Laarhoven H W M
Cancer Center Amsterdam, Amsterdam, The Netherlands.
Department of Medical Oncology, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.
PLoS One. 2018 Feb 8;13(2):e0192310. doi: 10.1371/journal.pone.0192310. eCollection 2018.
Clinical prediction models are increasingly used to predict outcomes such as survival in cancer patients. The aim of this study was threefold. First, to perform a systematic review to identify available clinical prediction models for patients with esophageal and/or gastric cancer. Second, to evaluate sources of bias in the included studies. Third, to investigate the predictive performance of the prediction models using meta-analysis.
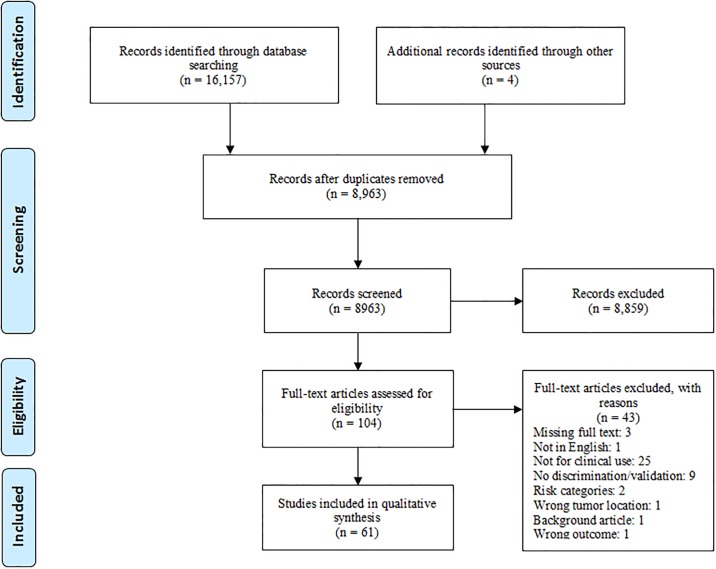
MEDLINE, EMBASE, PsycINFO, CINAHL, and The Cochrane Library were searched for publications from the year 2000 onwards. Studies describing models predicting survival, adverse events and/or health-related quality of life (HRQoL) for esophageal or gastric cancer patients were included. Potential sources of bias were assessed and a meta-analysis, pooled per prediction model, was performed on the discriminative abilities (c-indices).
A total of 61 studies were included (45 development and 16 validation studies), describing 47 prediction models. Most models predicted survival after a curative resection. Nearly 75% of the studies exhibited bias in at least 3 areas and model calibration was rarely reported. The meta-analysis showed that the averaged c-index of the models is fair (0.75) and ranges from 0.65 to 0.85.
Most available prediction models only focus on survival after a curative resection, which is only relevant to a limited patient population. Few models predicted adverse events after resection, and none focused on patient's HRQoL, despite its relevance. Generally, the quality of reporting is poor and external model validation is limited. We conclude that there is a need for prediction models that better meet patients' information needs, and provide information on both the benefits and harms of the various treatment options in terms of survival, adverse events and HRQoL.
临床预测模型越来越多地用于预测癌症患者的生存等结局。本研究有三个目的。第一,进行系统评价以识别食管癌和/或胃癌患者可用的临床预测模型。第二,评估纳入研究中的偏倚来源。第三,使用荟萃分析研究预测模型的预测性能。
检索MEDLINE、EMBASE、PsycINFO、CINAHL和考克兰图书馆自2000年起的出版物。纳入描述预测食管癌或胃癌患者生存、不良事件和/或健康相关生活质量(HRQoL)的模型的研究。评估潜在的偏倚来源,并对每个预测模型进行荟萃分析,分析其判别能力(c指数)。
共纳入61项研究(45项开发研究和16项验证研究),描述了47个预测模型。大多数模型预测根治性切除术后的生存情况。近75%的研究在至少3个方面存在偏倚,且很少报告模型校准情况。荟萃分析表明,模型的平均c指数为中等(0.75),范围为0.65至0.85。
大多数可用的预测模型仅关注根治性切除术后的生存情况,这仅与有限的患者群体相关。很少有模型预测切除术后的不良事件,且没有一个模型关注患者的HRQoL,尽管其具有相关性。总体而言,报告质量较差,外部模型验证有限。我们得出结论,需要有能更好满足患者信息需求的预测模型,并提供关于各种治疗方案在生存、不良事件和HRQoL方面的利弊信息。