Sgambat Kristen, Clauss Sarah, Moudgil Asha
Department of Nephrology, Children's National Medical Center, Washington, DC, USA.
Department of Cardiology, Children's National Medical center, Washington, DC, USA.
Clin Kidney J. 2018 Feb;11(1):136-146. doi: 10.1093/ckj/sfx056. Epub 2017 Jul 12.
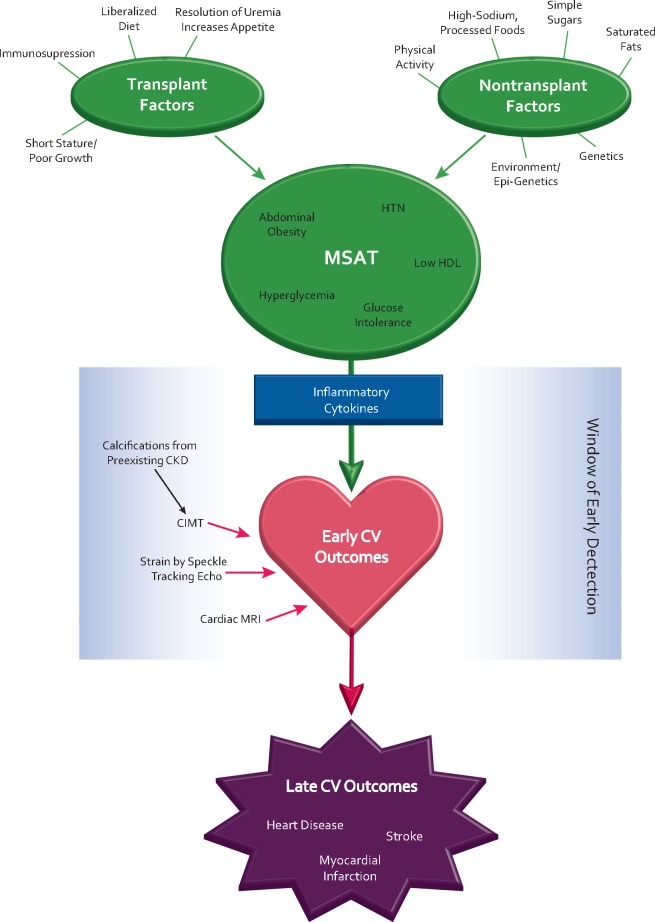
Children are at increased risk of developing metabolic syndrome (MS) after kidney transplantation, which contributes to long-term cardiovascular (CV) morbidities and decline in allograft function. While MS in the general population occurs due to excess caloric intake and physical inactivity, additional chronic kidney disease and transplant-related factors contribute to the development of MS in transplant recipients. Despite its significant health consequences, the interplay of the individual components in CV morbidity in pediatric transplant recipients is not well understood. Additionally, the optimal methods to detect early CV dysfunction are not well defined in this unique population. The quest to establish clear guidelines for diagnosis is further complicated by genetic differences among ethnic groups that necessitate the development of race-specific criteria, particularly with regard to individuals of African descent who carry the apolipoprotein L1 variant. In children, since major CV events are rare and traditional echocardiographic measures of systolic function, such as ejection fraction, are typically well preserved, the presence of CV disease often goes undetected in the early stages. Recently, new noninvasive imaging techniques have become available that offer the opportunity for early detection. Carotid intima-media thickness and impaired myocardial strain detected by speckle tracking echocardiography or cardiac magnetic resonance are emerging as early and sensitive markers of subclinical CV dysfunction. These highly sensitive tools may offer the opportunity to elucidate subtle CV effects of MS in children after transplantation. Current knowledge and future directions are explored in this review.
儿童肾移植后发生代谢综合征(MS)的风险增加,这会导致长期心血管(CV)疾病以及移植肾功能下降。虽然普通人群中的MS是由于热量摄入过多和缺乏身体活动引起的,但额外的慢性肾病和移植相关因素也会促使移植受者发生MS。尽管MS会产生严重的健康后果,但小儿移植受者中CV疾病各个组成部分之间的相互作用尚未得到充分了解。此外,在这个独特的人群中,检测早期CV功能障碍的最佳方法也没有明确界定。由于不同种族之间的基因差异,需要制定针对特定种族的标准,尤其是对于携带载脂蛋白L1变体的非洲裔个体,这使得制定明确的诊断指南变得更加复杂。在儿童中,由于主要的CV事件很少见,而且传统的收缩功能超声心动图测量指标,如射血分数,通常保持良好,因此CV疾病在早期往往未被发现。最近,新的非侵入性成像技术已经出现,为早期检测提供了机会。通过斑点追踪超声心动图或心脏磁共振检测到的颈动脉内膜中层厚度和心肌应变受损正在成为亚临床CV功能障碍的早期敏感标志物。这些高度敏感的工具可能为阐明移植后儿童MS的细微CV影响提供机会。本综述探讨了当前的知识和未来的方向。