Ibrahim Mohamed M, Poveromo Luke P, Glisson Richard R, Cornejo Agustin, Farjat Alfredo E, Gall Ken, Levinson Howard
Division of Plastic and Reconstructive Surgery, Department of Surgery, Duke University Medical Center, Durham, NC 27710, USA.
Duke University School of Medicine, Duke University Medical Center, Durham, NC 27710, USA.
J Biomech. 2018 Apr 11;71:43-51. doi: 10.1016/j.jbiomech.2018.01.022. Epub 2018 Feb 2.
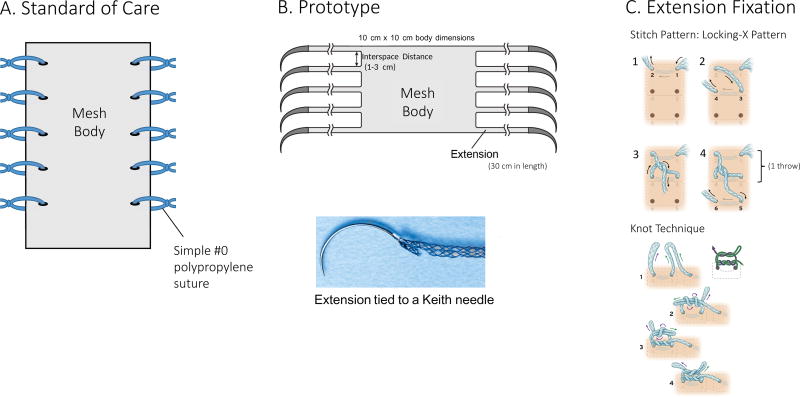
Approximately 348,000 ventral hernia repairs are performed annually in the United States and the incisional hernia recurrence rate is approximately 20% as a result of suture and mesh device failure. Device failure is related to changes at the suture/tissue interface that leads to acute or chronic suture pull-through and surgical failure. To better manage mechanical tension, we propose a modified mesh design with extensions and demonstrate its mechanical superiority.
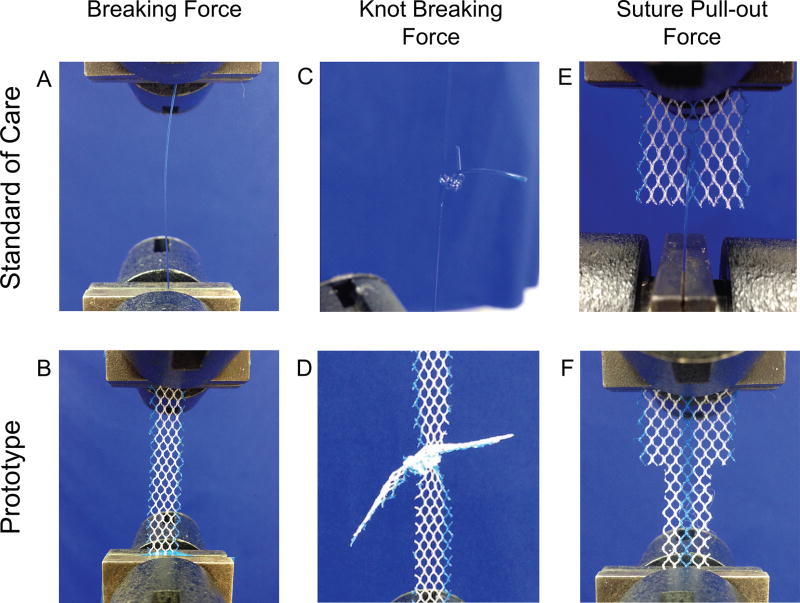
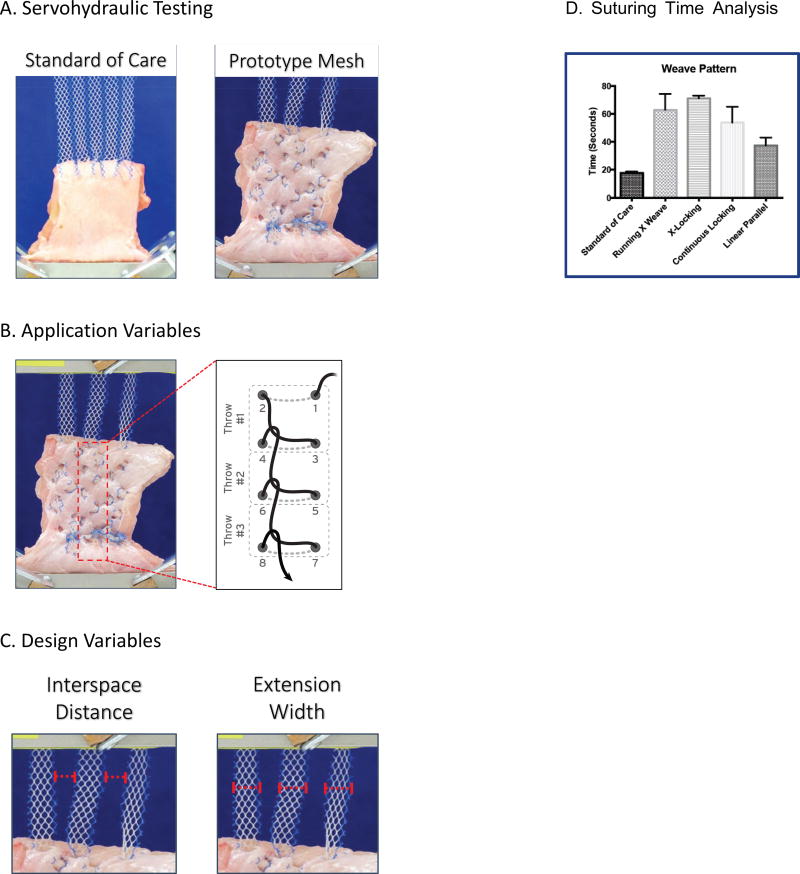
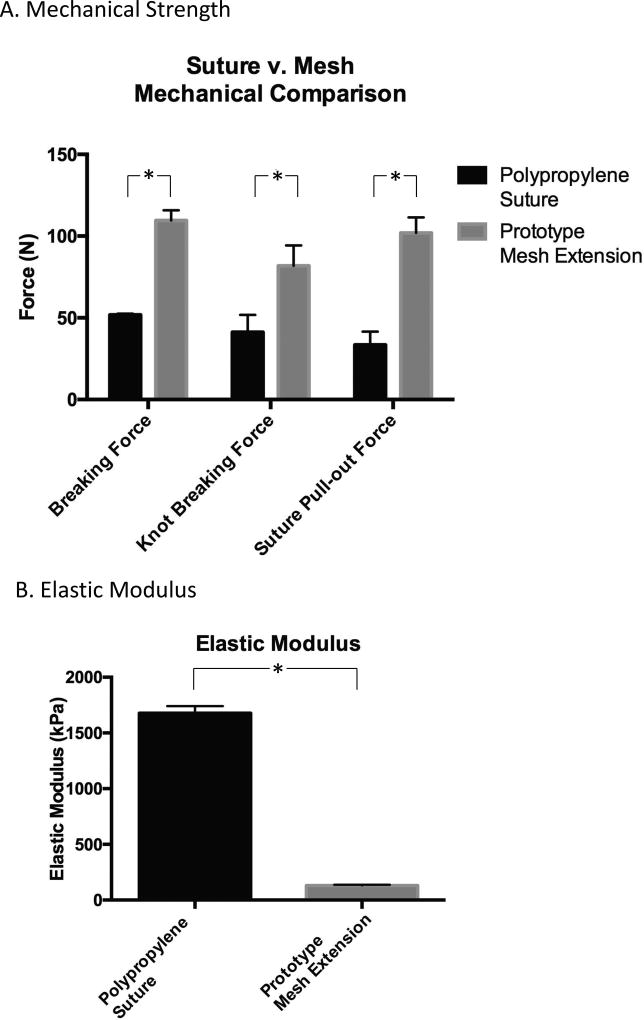
Comparative uniaxial static tensile testing was conducted on polypropylene suture and a modified mesh. Subsequently, a standard of care (SOC) mesh and modified mesh were evaluated using a tensometer in an acute hernia bench-top model.
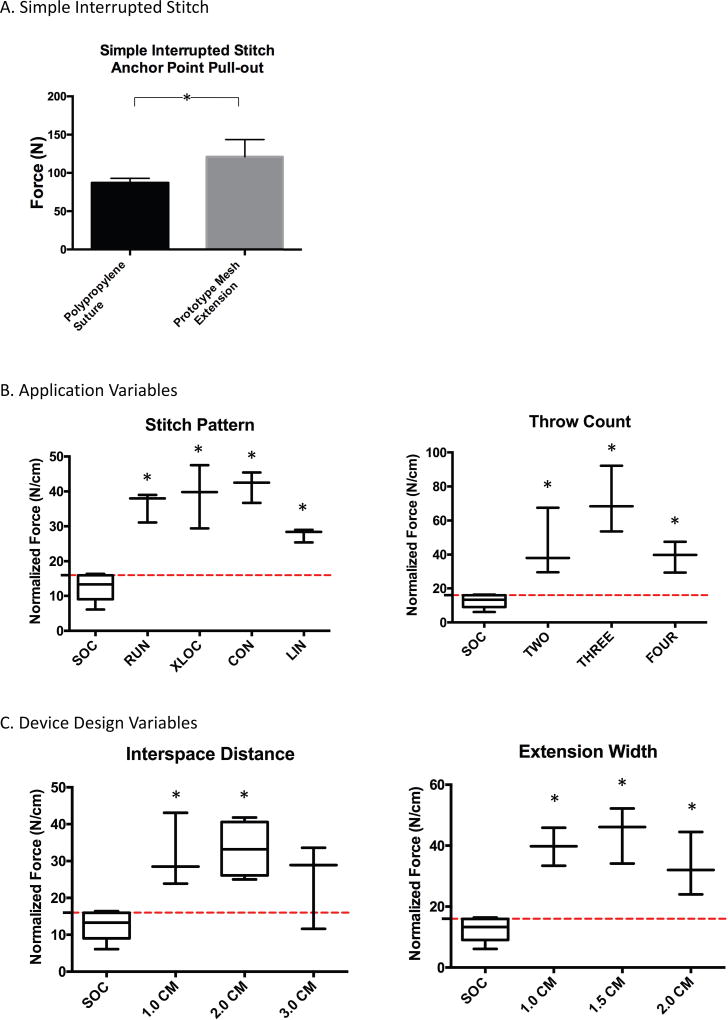
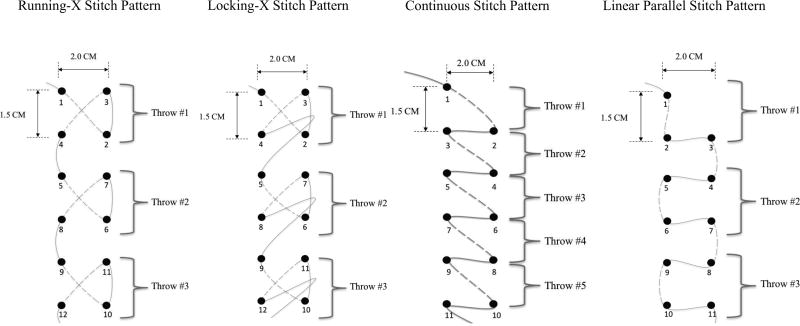
Modified mesh breaking strength, extension knot breaking strength, extension disruption, and extension anchoring were superior to suture (p < .05). Modified mesh ultimate tensile strength of anchoring was superior to SOC mesh (p < .05). Various stitch patterns and modifications in device design significantly improved device tension-free performance far beyond clinically relevant benchmarks (p < .05).
Testing demonstrates that the modified mesh outperforms SOC mesh and suture in all tested failure modes. SOC hernia mesh tears through tissue at stress levels below maximum physiologic stress, whereas, the modified hernia mesh is up to 200% stronger than SOC mesh at resisting suture tearing through tissue and maintains anchoring at stresses far beyond clinically relevant benchmarks. Modifying hernia mesh design significantly improves device mechanical performance and enhances tension-free repair.
在美国,每年大约进行348,000例腹疝修补术,由于缝合线和补片装置失效,切口疝复发率约为20%。装置失效与缝合线/组织界面的变化有关,这会导致急性或慢性缝合线拉出和手术失败。为了更好地管理机械张力,我们提出了一种带有延伸部分的改良补片设计,并展示其机械优势。
对聚丙烯缝合线和改良补片进行了比较单轴静态拉伸试验。随后,在急性疝台式模型中使用张力计对标准护理(SOC)补片和改良补片进行评估。
改良补片的断裂强度、延伸结断裂强度、延伸破坏和延伸锚固均优于缝合线(p<0.05)。改良补片锚固的极限抗拉强度优于SOC补片(p<0.05)。各种缝合模式和装置设计的改进显著提高了装置的无张力性能,远远超出临床相关基准(p<0.05)。
测试表明,在所有测试的失效模式下,改良补片均优于SOC补片和缝合线。SOC疝补片在应力水平低于最大生理应力时会撕裂组织,而改良疝补片在抵抗缝合线撕裂组织方面比SOC补片强200%,并且在远远超出临床相关基准的应力下仍能保持锚固。改良疝补片设计显著提高了装置的机械性能并增强了无张力修复效果。