Shah Shalin, Wood Kevin, Labadie Brian, Won Brian, Brisson Ryan, Karrison Theodore, Hensing Thomas, Kozloff Mark, Bao Riyue, Patel Jyoti D, Luke Jason J
Department of Medicine, NorthShore University HealthSystems, Chicago, IL, USA.
Department of Medicine, University of Chicago, Chicago, IL, USA.
Oncotarget. 2017 Dec 15;9(4):4375-4384. doi: 10.18632/oncotarget.23315. eCollection 2018 Jan 12.
The majority of non-small cell lung cancer (NSCLC) patients treated with anti-PD-1/PD-L1 therapy develop either innate or acquired resistance. Across tumor types, the "T cell-inflamed" tumor microenvironment correlates with clinical response to immunotherapy. We hypothesize that clinical characteristics may be predictive of resistance and that "T cell-inflamed" NSCLC tumors can be identified by gene expression profiling.
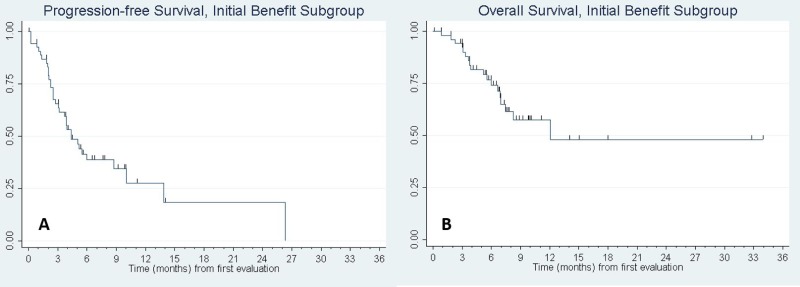
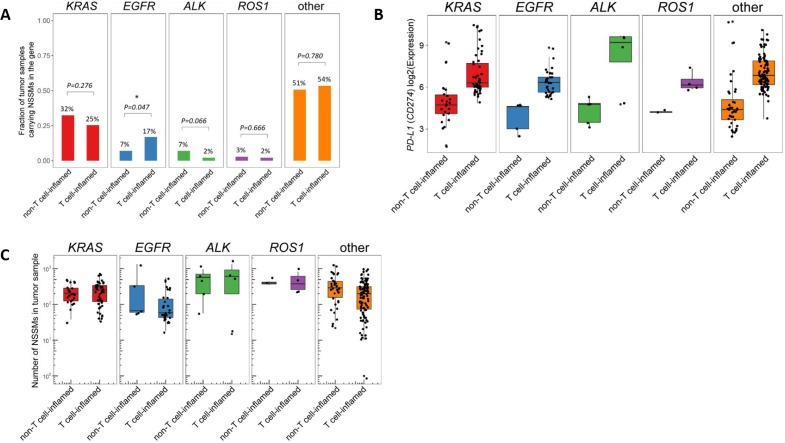
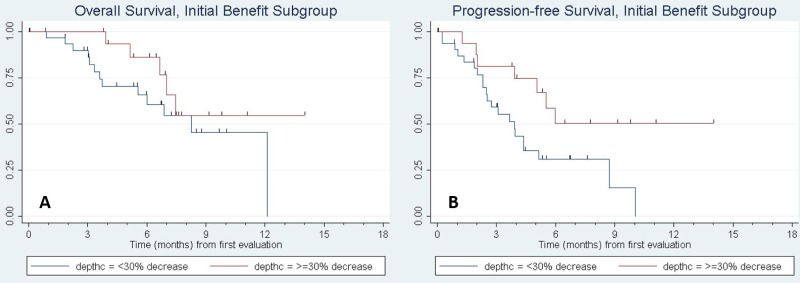
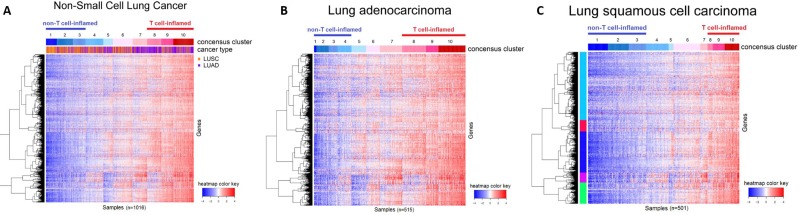
Of 93 patients, 36 (38.7%) had innate resistance and 57 (61.3%) had initial benefit to immunotherapy. Innate resistance was associated with non-smokers ( = 0.013), more involved disease sites ( = 0.011), more prior therapy ( = 0.001), and a lower albumin level ( = 0.014). Among patients with initial benefit, factors associated with subsequent progression-free survival included higher Karnofsky Performance Status (KPS) ( = 0.004) and lower depth of response to anti-PD-1 therapy ( = 0.003). A "T cell-inflamed" microenvironment was identified in 42% of TCGA adenocarcinoma samples versus 21.0% of squamous cell.
Specific clinical characteristics appear to be predictive of either innate or acquired resistance to anti-PD-1/PD-L1 therapy. A "T cell-inflamed" tumor was more common in adenocarcinoma than squamous histology.
A retrospective review of NSCLC patients treated with anti-PD-1/PD-L1 monotherapy. Patients with innate resistance to anti-PD-1/PD-L1 therapy (defined as progression at first CT evaluation) were compared to patients with initial clinical benefit. Among those with initial clinical benefit, we identified prognostic factors for time to progression (acquired resistance) or death. To further corroborate our findings on limited numbers, immune gene expression profiling of all NSCLC samples from the TCGA database was also pursued.
大多数接受抗PD-1/PD-L1治疗的非小细胞肺癌(NSCLC)患者会产生先天性或获得性耐药。在各种肿瘤类型中,“T细胞炎症性”肿瘤微环境与免疫治疗的临床反应相关。我们假设临床特征可能预测耐药性,并且“T细胞炎症性”NSCLC肿瘤可通过基因表达谱进行识别。
93例患者中,36例(38.7%)有先天性耐药,57例(61.3%)对免疫治疗有初始获益。先天性耐药与不吸烟者相关(P = 0.013)、疾病累及部位更多(P = 0.011)、既往治疗更多(P = 0.001)以及白蛋白水平较低(P = 0.014)。在有初始获益的患者中,与后续无进展生存期相关的因素包括较高的卡诺夫斯基表现状态(KPS)(P = 0.004)和较低的抗PD-1治疗反应深度(P = 0.003)。42%的TCGA腺癌样本中鉴定出“T细胞炎症性”微环境,而鳞状细胞样本中为21.0%。
特定临床特征似乎可预测对抗PD-1/PD-L1治疗的先天性或获得性耐药。“T细胞炎症性 ”肿瘤在腺癌中比鳞状组织学中更常见。
对接受抗PD-1/PD-L1单药治疗的NSCLC患者进行回顾性研究。将对抗PD-1/PD-L1治疗有先天性耐药的患者(定义为首次CT评估时进展)与有初始临床获益的患者进行比较。在有初始临床获益的患者中,我们确定了进展时间(获得性耐药)或死亡的预后因素。为了进一步证实我们在有限数量上的发现,还对来自TCGA数据库的所有NSCLC样本进行了免疫基因表达谱分析。