Choi Sanghun, Haghighi Babak, Choi Jiwoong, Hoffman Eric A, Comellas Alejandro P, Newell John D, Wenzel Sally E, Castro Mario, Fain Sean B, Jarjour Nizar N, Schiebler Mark L, Barr R Graham, Han MeiLan K, Bleecker Eugene R, Cooper Christopher B, Couper David, Hansel Nadia, Kanner Richard E, Kazerooni Ella A, Kleerup Eric A C, Martinez Fernando J, O'Neal Wanda K, Woodruff Prescott G, Lin Ching-Long
Department of Mechanical Engineering, Kyungpook National University, Daegu, South Korea.
Department of Mechanical and Industrial Engineering, University of Iowa, Iowa City, Iowa, USA.
BMJ Open Respir Res. 2017 Nov 9;4(1):e000252. doi: 10.1136/bmjresp-2017-000252. eCollection 2017.
Quantitative CT (QCT) imaging-based metrics have quantified disease alterations in asthma and chronic obstructive pulmonary disease (COPD), respectively. We seek to characterise the similarity and disparity between these groups using QCT-derived airway and parenchymal metrics.
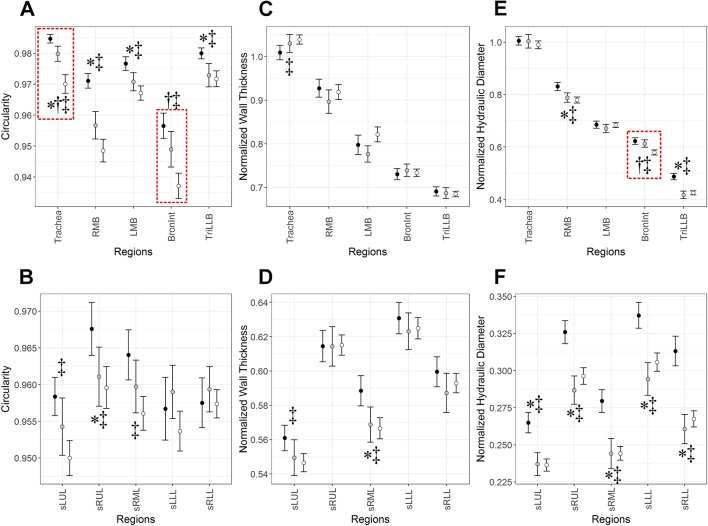
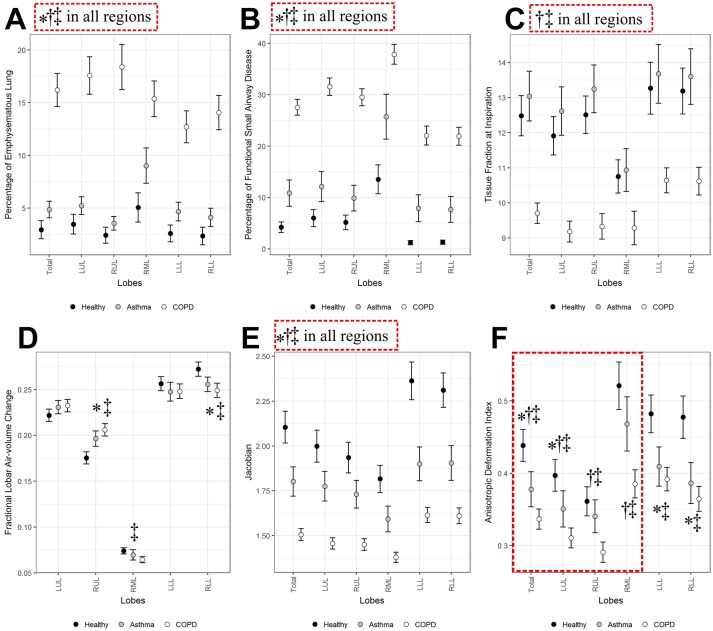
Asthma and COPD subjects (former-smoker status) were selected with a criterion of post-bronchodilator FEV <80%. Healthy non-smokers were included as a control group. Inspiratory and expiratory QCT images of 75 asthmatic, 215 COPD and 94 healthy subjects were evaluated. We compared three segmental variables: airway circularity, normalised wall thickness and normalised hydraulic diameter, indicating heterogeneous airway shape, wall thickening and luminal narrowing, respectively. Using an image registration, we also computed six lobar variables including per cent functional small-airway disease, per cent emphysema, tissue fraction at inspiration, fractional-air-volume change, Jacobian and functional metric characterising anisotropic deformation.
Compared with healthy subjects, both asthma and COPD subjects demonstrated a decreased airway circularity especially in large and upper lobar airways, and a decreased normalised hydraulic diameter in segmental airways. Besides, COPD subjects had more severe emphysema and small-airway disease, as well as smaller regional tissue fraction and lung deformation, compared with asthmatic subjects. The difference of emphysema, small-airway disease and tissue fraction between asthma and COPD was more prominent in upper and middle lobes.
Patients with asthma and COPD, with a persistent FEV <80%, demonstrated similar alterations in airway geometry compared with controls, but different degrees of alterations in parenchymal regions. Density-based metrics measured at upper and middle lobes were found to be discriminant variables between patients with asthma and COPD.
基于定量CT(QCT)成像的指标已分别对哮喘和慢性阻塞性肺疾病(COPD)中的疾病改变进行了量化。我们试图使用QCT得出的气道和实质指标来描述这些组之间的异同。
选择哮喘和COPD受试者(既往吸烟状况),其标准为支气管扩张剂后FEV<80%。纳入健康非吸烟者作为对照组。对75例哮喘患者、215例COPD患者和94例健康受试者的吸气和呼气QCT图像进行评估。我们比较了三个节段变量:气道圆度、标准化壁厚和标准化水力直径,分别表示气道形状不均一、壁增厚和管腔狭窄。通过图像配准,我们还计算了六个肺叶变量,包括功能性小气道疾病百分比、肺气肿百分比、吸气时的组织分数、空气体积分数变化、雅可比行列式和表征各向异性变形的功能指标。
与健康受试者相比,哮喘和COPD受试者均表现出气道圆度降低,尤其是在大叶和上叶气道,节段气道的标准化水力直径也降低。此外,与哮喘受试者相比,COPD受试者的肺气肿和小气道疾病更严重,区域组织分数和肺变形更小。哮喘和COPD在肺气肿、小气道疾病和组织分数方面的差异在上叶和中叶更为突出。
FEV持续<80%的哮喘和COPD患者与对照组相比,在气道几何形状上表现出相似的改变,但在实质区域的改变程度不同。发现在上叶和中叶测量的基于密度的指标是哮喘和COPD患者之间的判别变量。