Department of Surgery, VU University Medical Center, Amsterdam, The Netherlands.
IRCAD/ EITS, Department of General, Digestive and Endocrine Surgery, Nouvel Hôpital Civil, University Hospital of Strasbourg, Strasbourg, France.
Surg Endosc. 2018 Aug;32(8):3582-3591. doi: 10.1007/s00464-018-6086-3. Epub 2018 Feb 12.
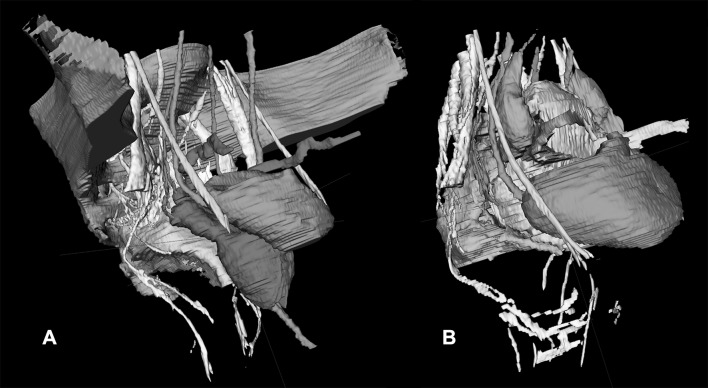
Long-term morbidity after multimodal treatment for rectal cancer is suggested to be mainly made up by nerve-injury-related dysfunctions. Stereotactic navigation for rectal surgery was shown to be feasible and will be facilitated by highlighting structures at risk of iatrogenic damage. The aim of this study was to investigate the ability to make a 3D map of the pelvic nerves with magnetic resonance imaging (MRI).
A systematic review was performed to identify a main positional reference for each pelvic nerve and plexus. The nerves were manually delineated in 20 volunteers who were scanned with a 3-T MRI. The nerve identifiability rate and the likelihood of nerve identification correctness were determined.
The analysis included 61 studies on pelvic nerve anatomy. A main positional reference was defined for each nerve. On MRI, the sacral nerves, the lumbosacral plexus, and the obturator nerve could be identified bilaterally in all volunteers. The sympathetic trunk could be identified in 19 of 20 volunteers bilaterally (95%). The superior hypogastric plexus, the hypogastric nerve, and the inferior hypogastric plexus could be identified bilaterally in 14 (70%), 16 (80%), and 14 (70%) of the 20 volunteers, respectively. The pudendal nerve could be identified in 17 (85%) volunteers on the right side and in 13 (65%) volunteers on the left side. The levator ani nerve could be identified in only a few volunteers. Except for the levator ani nerve, the radiologist and the anatomist agreed that the delineated nerve depicted the correct nerve in 100% of the cases.
Pelvic nerves at risk of injury are usually visible on high-resolution MRI with dedicated scanning protocols. A specific knowledge of their course and its application in stereotactic navigation is suggested to improve quality of life by decreasing the likelihood of nerve injury.
多模态治疗直肠癌后的长期发病率主要由神经损伤相关的功能障碍构成。直肠手术的立体定向导航已被证明是可行的,并将通过突出易发生医源性损伤的结构而得到促进。本研究旨在调查使用磁共振成像(MRI)制作骨盆神经 3D 图谱的能力。
系统评价旨在确定每个骨盆神经和神经丛的主要位置参考。对 20 名志愿者进行了 3T MRI 扫描,手动勾画了这些神经。确定了神经可识别率和神经识别正确性的可能性。
分析包括 61 项关于骨盆神经解剖结构的研究。为每条神经定义了主要位置参考。在 MRI 上,所有志愿者双侧均可识别出骶神经、腰骶丛和闭孔神经。交感干双侧可在 19 名志愿者中识别(95%)。双侧可在 14 名志愿者中识别出 14 名(70%)、16 名(80%)和 14 名(70%)的腹下丛、腹下神经和下腹下丛。右侧 17 名(85%)志愿者和左侧 13 名(65%)志愿者可识别阴部神经。只有少数志愿者可以识别肛提肌神经。除肛提肌神经外,放射科医生和解剖学家一致认为,在 100%的病例中,勾画的神经描绘了正确的神经。
具有专用扫描方案的高分辨率 MRI 通常可显示易受伤的骨盆神经。建议特定了解其行程及其在立体定向导航中的应用,以通过降低神经损伤的可能性来提高生活质量。