Lee Jeongshim, Ahn Sung Soo, Chang Jong Hee, Suh Chang Ok
Department of Radiation Oncology, Yonsei University College of Medicine, Seoul, Korea.
Department of Radiation Oncology, Inha University Hospital, Incheon, Korea.
Yonsei Med J. 2018 Mar;59(2):194-201. doi: 10.3349/ymj.2018.59.2.194.
To evaluate the adequacy of retreatment, including hypofractionated re-irradiation (HFReRT), after surgery for recurrent glioblastoma (GBM) and related prognosticators of outcomes.
From 2011 to 2014, 25 consecutive patients with recurrent (n=17) or secondary (n=7) disease underwent maximal surgery and subsequent HFReRT after meeting the following conditions: 1) confirmation of recurrent or secondary GBM after salvage surgery; 2) Karnofsky performance score (KPS) ≥60; and 3) interval of ≥12 months between initial radiotherapy and HFReRT. HFReRT was delivered using a simultaneous integrated boost technique, with total dose of 45 Gy in 15 fractions to the gross tumor volume (GTV) and 37.5 Gy in 15 fractions to the clinical target volume.
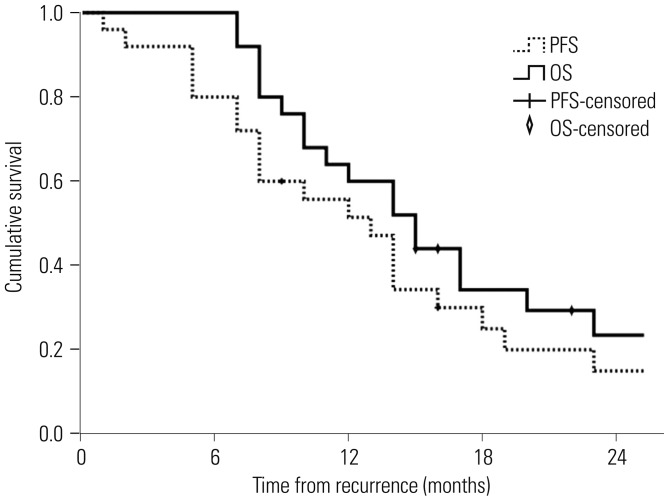
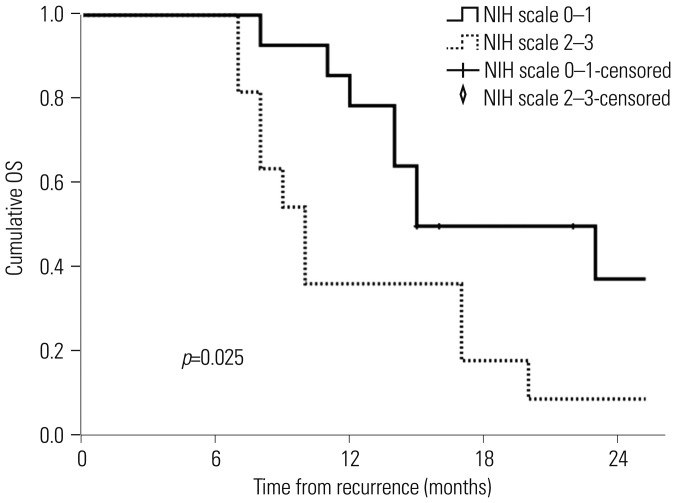
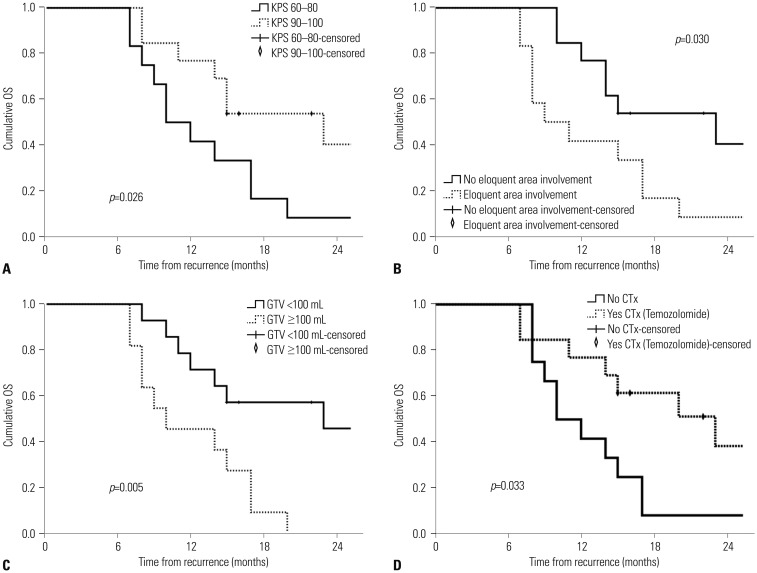
During a median follow-up of 13 months, the median progression-free and overall survival (OS) were 13 and 16 months, respectively. A better KPS (p=0.026), no involvement of the eloquent area at recurrence (p=0.030), and a smaller GTV (p=0.005) were associated with better OS. Additionally, OS differed significantly between risk groups stratified by the National Institutes of Health Recurrent GBM Scale (low-risk vs. high-risk, p=0.025). Radiologically suspected radiation necrosis (RN) was observed in 16 patients (64%) at a median of 9 months after HFReRT, and 8 patients developed grade 3 RN requiring hospitalization.
HFReRT after maximal surgery prolonged survival in selected patients with recurrent GBM, especially those with small-sized recurrences in non-eloquent areas and good performance.
评估复发性胶质母细胞瘤(GBM)术后再治疗的充分性,包括低分割再照射(HFReRT)以及相关的预后指标。
2011年至2014年,25例连续的复发性(n = 17)或继发性(n = 7)疾病患者在满足以下条件后接受了最大程度的手术及随后的HFReRT:1)挽救性手术后复发性或继发性GBM得到确认;2)卡诺夫斯基性能评分(KPS)≥60;3)初始放疗与HFReRT之间的间隔≥12个月。HFReRT采用同步整合加量技术,给予大体肿瘤体积(GTV)45 Gy,分15次照射,临床靶体积37.5 Gy,分15次照射。
在中位随访13个月期间,中位无进展生存期和总生存期(OS)分别为13个月和16个月。较好的KPS(p = 0.026)、复发时未累及功能区(p = 0.030)以及较小的GTV(p = 0.005)与较好的OS相关。此外,根据美国国立卫生研究院复发性GBM量表分层的风险组之间OS有显著差异(低风险与高风险,p = 0.025)。在HFReRT后中位9个月时,16例患者(64%)出现放射学怀疑的放射性坏死(RN),8例患者发生3级RN需要住院治疗。
最大程度手术后的HFReRT延长了部分复发性GBM患者的生存期,尤其是那些非功能区小复发且状态良好的患者。