Department of Endocrinology and Metabolism, Academic Medical Center, Amsterdam, The Netherlands.
Department of Internal Medicine I, Division of Nephrology and Cardiology, Comprehensive Heart Failure Center (CHFC) and Fabry Center for Interdisciplinary Therapy (FAZIT), University Hospital Wuerzburg, Wuerzburg, Germany.
J Med Genet. 2018 May;55(5):351-358. doi: 10.1136/jmedgenet-2017-104863. Epub 2018 Feb 7.
Two recombinant enzymes (agalsidase alfa 0.2 mg/kg/every other week and agalsidase beta 1.0 mg/kg/every other week) have been registered for the treatment of Fabry disease (FD), at equal high costs. An independent international initiative compared clinical and biochemical outcomes of the two enzymes.
In this multicentre retrospective cohort study, clinical event rate, left ventricular mass index (LVMI), estimated glomerular filtration rate (eGFR), antibody formation and globotriaosylsphingosine (lysoGb3) levels were compared between patients with FD treated with agalsidase alfa and beta at their registered dose after correction for phenotype and sex.
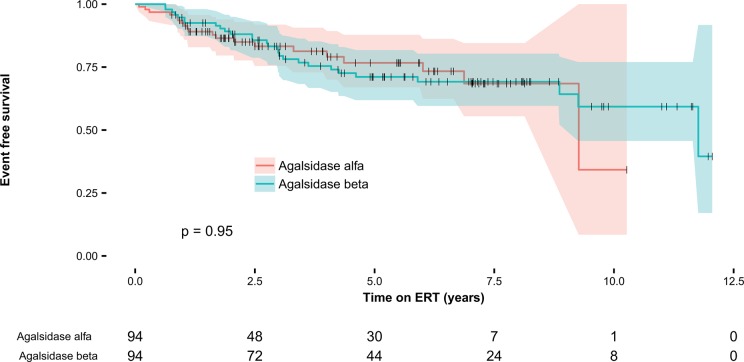
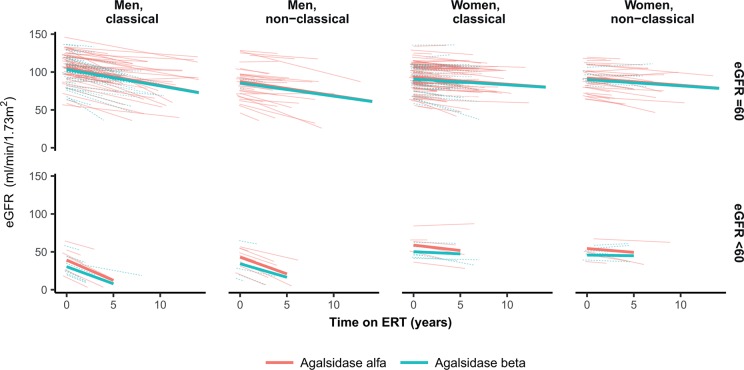
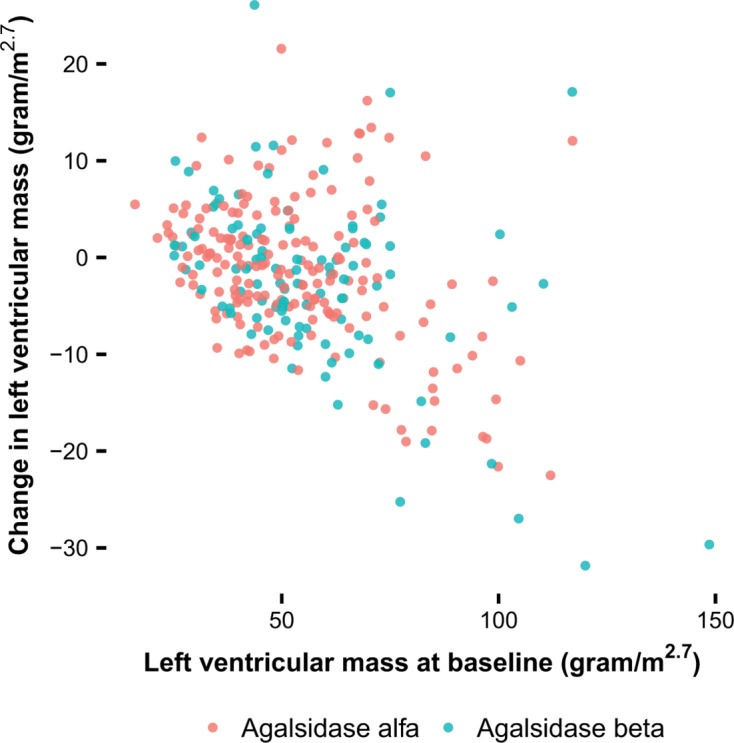
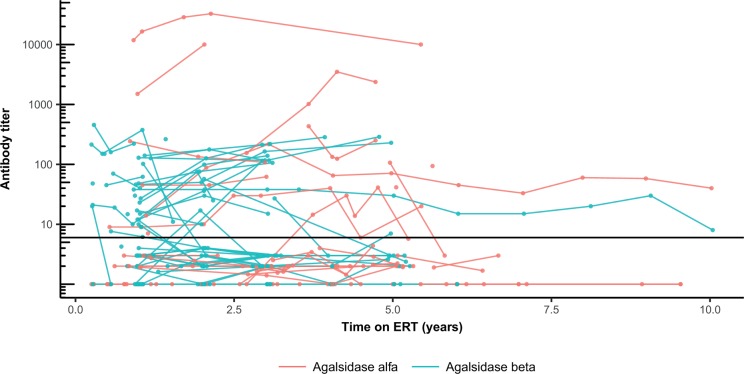
387 patients (192 women) were included, 248 patients received agalsidase alfa. Mean age at start of enzyme replacement therapy was 46 (±15) years. Propensity score matched analysis revealed a similar event rate for both enzymes (HR 0.96, P=0.87). The decrease in plasma lysoGb3 was more robust following treatment with agalsidase beta, specifically in men with classical FD (β: -18 nmol/L, P<0.001), persisting in the presence of antibodies. The risk to develop antibodies was higher for patients treated with agalsidase beta (OR 2.8, P=0.04). LVMI decreased in a higher proportion following the first year of agalsidase beta treatment (OR 2.27, P=0.03), while eGFR slopes were similar.
Treatment with agalsidase beta at higher dose compared with agalsidase alfa does not result in a difference in clinical events, which occurred especially in those with more advanced disease. A greater biochemical response, also in the presence of antibodies, and better reduction in left ventricular mass was observed with agalsidase beta.
两种重组酶(阿加糖酶α 0.2mg/kg,每两周一次;阿加糖酶β 1.0mg/kg,每两周一次)已被注册用于治疗 Fabry 病(FD),费用相同。一个独立的国际倡议比较了这两种酶的临床和生化结果。
在这项多中心回顾性队列研究中,比较了接受阿加糖酶α和β治疗的 FD 患者在纠正表型和性别后,以注册剂量治疗时的临床事件发生率、左心室质量指数(LVMI)、估计肾小球滤过率(eGFR)、抗体形成和神经酰胺三己糖苷(lysoGb3)水平。
纳入 387 例患者(192 例女性),其中 248 例接受阿加糖酶α治疗。酶替代治疗开始时的平均年龄为 46(±15)岁。倾向评分匹配分析显示两种酶的事件发生率相似(HR 0.96,P=0.87)。阿加糖酶β治疗后,血浆 lysoGb3 的下降更为显著,尤其是在经典 FD 男性中(β:-18nmol/L,P<0.001),且持续存在抗体。与接受阿加糖酶α治疗的患者相比,接受阿加糖酶β治疗的患者发生抗体的风险更高(OR 2.8,P=0.04)。阿加糖酶β治疗第一年,LVMI 下降的比例更高(OR 2.27,P=0.03),而 eGFR 斜率相似。
与阿加糖酶α相比,用更高剂量的阿加糖酶β治疗不会导致临床事件的差异,这些事件主要发生在疾病更严重的患者中。与阿加糖酶α相比,阿加糖酶β观察到更大的生化反应,即使存在抗体,左心室质量的减少也更好。