Misango David, Pattnaik Rajyabardhan, Baker Tim, Dünser Martin W, Dondorp Arjen M, Schultz Marcus J
Department of Anaesthesiology and Critical Care Medicine, Aga Khan University Hospital, Nairobi, Kenya.
Department of Intensive Care Medicine, Ispat General Hospital, Rourkela, Sundargarh, Odisha, India.
Trans R Soc Trop Med Hyg. 2017 Nov 1;111(11):483-489. doi: 10.1093/trstmh/try007.
Recommendations for haemodynamic assessment and support in sepsis and septic shock in resource-limited settings are largely lacking.
A task force of six international experts in critical care medicine, all of them members of the Global Intensive Care Working Group of the European Society of Intensive Care Medicine and with extensive bedside experience in resource-limited intensive care units, reviewed the literature and provided recommendations regarding haemodynamic assessment and support, keeping aspects of efficacy and effectiveness, availability and feasibility and affordability and safety in mind.
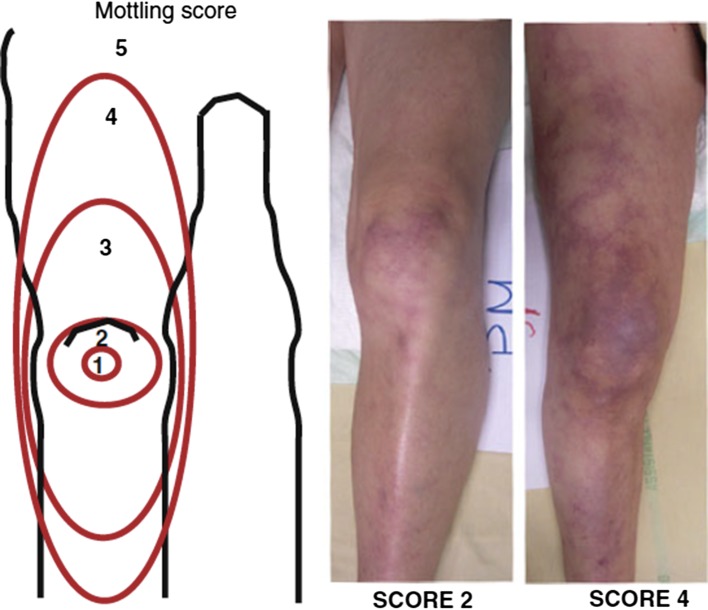
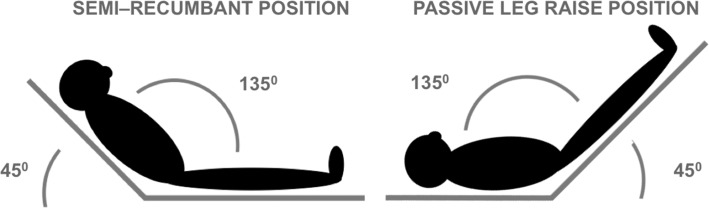
We suggest using capillary refill time, skin mottling scores and skin temperature gradients; suggest a passive leg raise test to guide fluid resuscitation; recommend crystalloid solutions as the initial fluid of choice; recommend initial fluid resuscitation with 30 ml/kg in the first 3 h, but with extreme caution in settings where there is a lack of mechanical ventilation; recommend against an early start of vasopressors; suggest starting a vasopressor in patients with persistent hypotension after initial fluid resuscitation with at least 30 ml/kg, but earlier when there is lack of vasopressors and mechanical ventilation; recommend using norepinephrine (noradrenaline) as a first-line vasopressor; suggest starting an inotrope with persistence of plasma lactate >2 mmol/L or persistence of skin mottling or prolonged capillary refill time when plasma lactate cannot be measured, and only after initial fluid resuscitation; suggest the use of dobutamine as a first-line inotrope; recommend administering vasopressors through a central venous line and suggest administering vasopressors and inotropes via a central venous line using a syringe or infusion pump when available.
Recommendations for haemodynamic assessment and support in sepsis and septic shock in resource-limited settings have been developed by a task force of six international experts in critical care medicine with extensive practical experience in resource-limited settings.
资源有限地区在脓毒症和脓毒性休克的血流动力学评估与支持方面,很大程度上缺乏相关建议。
一个由六位国际重症医学专家组成的特别工作组,他们均为欧洲重症医学会全球重症监护工作组的成员,且在资源有限的重症监护病房拥有丰富的床边经验,对文献进行了回顾,并就血流动力学评估与支持提出了建议,同时兼顾疗效、有效性、可及性、可行性、可负担性及安全性等方面。
我们建议使用毛细血管再充盈时间、皮肤花斑评分和皮肤温度梯度;建议进行被动抬腿试验以指导液体复苏;推荐晶体溶液作为初始首选液体;建议在最初3小时内按30ml/kg进行初始液体复苏,但在缺乏机械通气的情况下要极度谨慎;建议不要过早开始使用血管升压药;建议在初始液体复苏至少30ml/kg后仍持续低血压的患者中开始使用血管升压药,但在缺乏血管升压药和机械通气时可更早开始;推荐使用去甲肾上腺素作为一线血管升压药;建议在血浆乳酸持续>2mmol/L或持续出现皮肤花斑或在无法测量血浆乳酸时毛细血管再充盈时间延长且仅在初始液体复苏后开始使用正性肌力药物;建议使用多巴酚丁胺作为一线正性肌力药物;推荐通过中心静脉导管给予血管升压药,并建议在有条件时使用注射器或输液泵通过中心静脉导管给予血管升压药和正性肌力药物。
由六位在资源有限地区拥有丰富实践经验的国际重症医学专家组成的特别工作组,制定了资源有限地区脓毒症和脓毒性休克血流动力学评估与支持的建议。