Bittner George D, Sengelaub Dale R, Ghergherehchi Cameron L
Department of Neuroscience, University of Texas at Austin, Austin, TX, USA.
Department of Psychological and Brain Sciences, Indiana University, Bloomington, IN, USA.
Neural Regen Res. 2018 Jan;13(1):53-57. doi: 10.4103/1673-5374.224363.
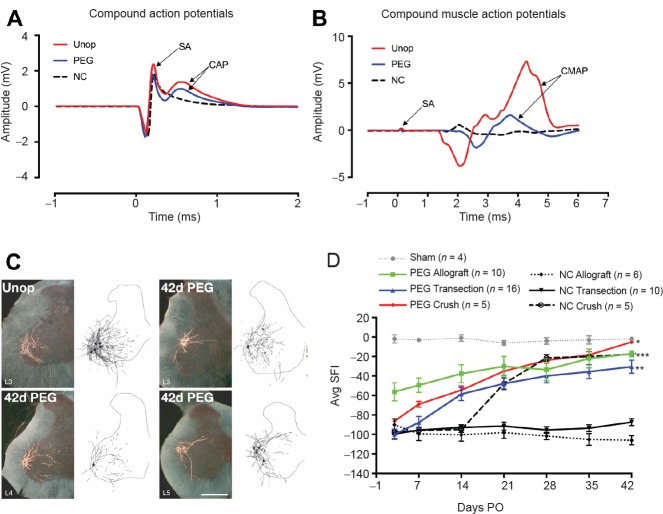
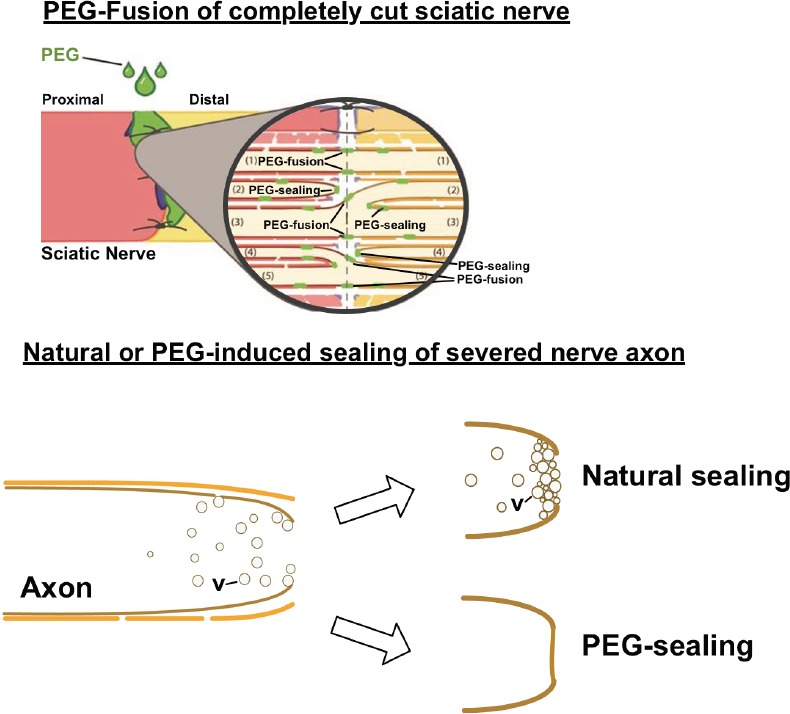
Current Neuroscience dogma holds that transections or ablations of a segment of peripheral nerves produce: (1) Immediate loss of axonal continuity, sensory signaling, and motor control; (2) Wallerian rapid (1-3 days) degeneration of severed distal axons, muscle atrophy, and poor behavioral recovery after many months (if ever, after ablations) by slowly-regenerating (1 mm/d), proximal-stump outgrowths that must specifically reinnervate denervated targets; (3) Poor acceptance of microsutured nerve allografts, even if tissue-matched and immune-suppressed. Repair of transections/ablations by neurorrhaphy and well-specified-sequences of PEG-fusion solutions (one containing polyethylene glycol, PEG) successfully address these problems. However, conundrums and confusions regarding unorthodox and dramatic results of PEG-fusion repair in animal model systems often lead to misunderstandings. For example, (1) Axonal continuity and signaling is re-established within minutes by non-specifically PEG-fusing (connecting) severed motor and sensory axons across each lesion site, but remarkable behavioral recovery to near-unoperated levels takes several weeks; (2) Many distal stumps of inappropriately-reconnected, PEG-fused axons do not ever (Wallerian) degenerate and continuously innervate muscle fibers that undergo much less atrophy than otherwise-denervated muscle fibers; (3) Host rats do not reject PEG-fused donor nerve allografts in a non-immuno-privileged environment with no tissue matching or immunosuppression; (4) PEG fuses apposed open axonal ends or seals each shut (thereby preventing PEG-fusion), depending on the experimental protocol; (5) PEG-fusion protocols produce similar results in animal model systems and early human case studies. Hence, iconoclastic PEG-fusion data appropriately understood might provoke a re-thinking of some Neuroscience dogma and a paradigm shift in clinical treatment of peripheral nerve injuries.
当前神经科学的教条认为,外周神经某一段的横断或切除会产生:(1)轴突连续性、感觉信号传导和运动控制立即丧失;(2)切断的远端轴突发生华勒氏快速(1 - 3天)变性、肌肉萎缩,并且在数月后(如果是切除后的情况,可能永远无法恢复)行为恢复不佳,这是因为近端残端以缓慢再生速度(1毫米/天)长出,必须特异性地重新支配失神经支配的靶点;(3)即使进行了组织匹配和免疫抑制,微缝合的神经同种异体移植的接受度也很差。通过神经缝合术和特定顺序的聚乙二醇融合溶液(一种含有聚乙二醇,PEG)修复横断/切除可以成功解决这些问题。然而,动物模型系统中聚乙二醇融合修复的非传统和显著结果所引发的难题和困惑常常导致误解。例如,(1)通过非特异性地将切断的运动和感觉轴突在每个损伤部位进行聚乙二醇融合(连接),轴突连续性和信号传导在数分钟内即可重建,但行为恢复到接近未手术水平则需要数周时间;(2)许多通过聚乙二醇融合不当重新连接的轴突的远端残端从未发生(华勒氏)变性,并持续支配肌肉纤维,这些肌肉纤维的萎缩程度远低于其他失神经支配的肌肉纤维;(3)在没有组织匹配或免疫抑制的非免疫特权环境中,宿主大鼠不会排斥聚乙二醇融合的供体神经同种异体移植;(4)根据实验方案,聚乙二醇会融合相对的开放轴突末端或封闭每个轴突末端(从而防止聚乙二醇融合);(5)聚乙二醇融合方案在动物模型系统和早期人类病例研究中产生了相似的结果。因此,正确理解这些打破传统的聚乙二醇融合数据可能会引发对一些神经科学教条的重新思考,并在外周神经损伤的临床治疗中引发范式转变。