Department of Medical Sciences, Cardiology, Uppsala University, Uppsala, Sweden.
Uppsala Clinical Research Center, Uppsala University, Uppsala, Sweden.
Heart. 2018 Aug;104(15):1284-1291. doi: 10.1136/heartjnl-2017-312409. Epub 2018 Feb 16.
The universal definition of myocardial infarction (MI) differentiates MI due to oxygen supply/demand mismatch (type 2) from MI due to plaque rupture (type 1) as well as from myocardial injuries of non-ischaemic or multifactorial nature. The purpose of this study was to investigate how often physicians agree in this classification and what factors lead to agreement or disagreement.
A total of 1328 patients diagnosed with MI at eight different Swedish hospitals 2011 were included. All patients were retrospectively reclassified into different MI or myocardial injury subtypes by two independent specially trained physicians, strictly adhering to the third universal definition of MI.
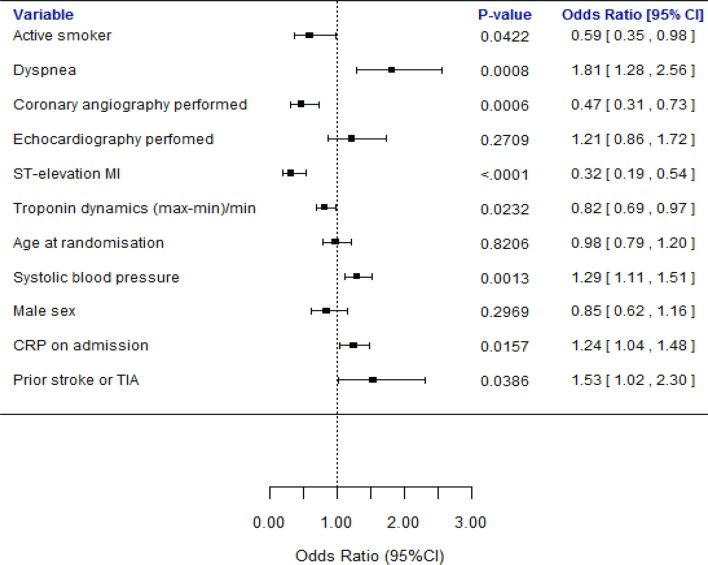
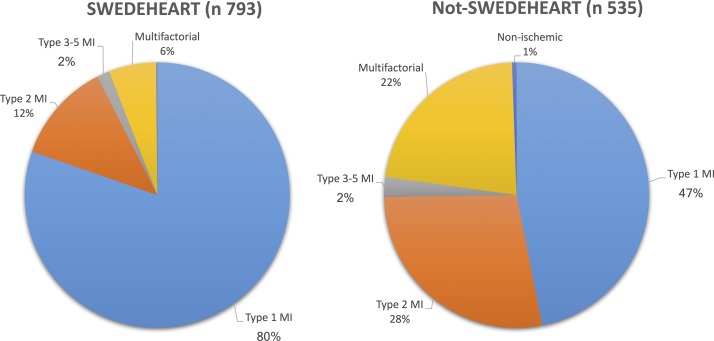
Overall, there was a moderate interobserver agreement with a kappa coefficient (κ) of 0.55 in this classification. There was substantial agreement when distinguishing type 1 MI (κ: 0.61), compared with moderate agreement when distinguishing type 2 MI (κ: 0.54). In multivariate logistic regression analyses, ST elevation MI (P<0.001), performed coronary angiography (P<0.001) and larger changes in troponin levels (P=0.023) independently made the physicians agree significantly more often, while they disagreed more often with symptoms of dyspnoea (P<0.001), higher systolic blood pressure (P=0.001) and higher C reactive protein levels on admission (P=0.016).
Distinguishing MI types is challenging also for trained adjudicators. Although strictly adhering to the third universal definition of MI, differentiation between type 1 MI, type 2 MI and myocardial injury only gave a moderate rate of interobserver agreement. More precise and clinically applicable criteria for the current classification, particularly for type 2 MI diagnosis, are urgently needed.
心肌梗死(MI)的通用定义将由于氧供需不匹配(2 型)引起的 MI 与由于斑块破裂(1 型)引起的 MI 以及非缺血性或多因素引起的心肌损伤区分开来。本研究旨在调查医生在这种分类中达成一致的频率,以及哪些因素导致了一致或不一致。
共纳入 2011 年在瑞典 8 家不同医院诊断为 MI 的 1328 例患者。所有患者均由两名独立的专门培训医生根据第三版 MI 通用定义进行回顾性重新分类为不同的 MI 或心肌损伤亚型。
总体而言,这种分类的观察者间一致性中等,kappa 系数(κ)为 0.55。在区分 1 型 MI 时,κ 值为 0.61,具有显著的一致性,而在区分 2 型 MI 时,κ 值为 0.54,具有中度一致性。在多变量逻辑回归分析中,ST 段抬高型 MI(P<0.001)、进行冠状动脉造影(P<0.001)和肌钙蛋白水平变化较大(P=0.023)可使医生更频繁地达成一致,而呼吸困难症状(P<0.001)、更高的收缩压(P=0.001)和入院时更高的 C 反应蛋白水平(P=0.016)则使医生更频繁地产生分歧。
即使是经过培训的裁判,区分 MI 类型也具有挑战性。尽管严格遵循 MI 的第三版通用定义,但区分 1 型 MI、2 型 MI 和心肌损伤仅产生中等程度的观察者间一致性。迫切需要更精确和临床适用的当前分类标准,特别是用于 2 型 MI 诊断的标准。