Department of Internal Medicine, National Taiwan University Hospital, No. 7, Chung-Shan South Road, Taipei, 100, Taiwan.
Mol Cancer. 2018 Feb 19;17(1):38. doi: 10.1186/s12943-018-0777-1.
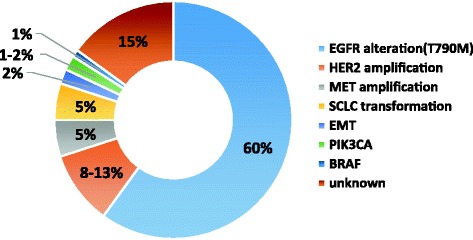
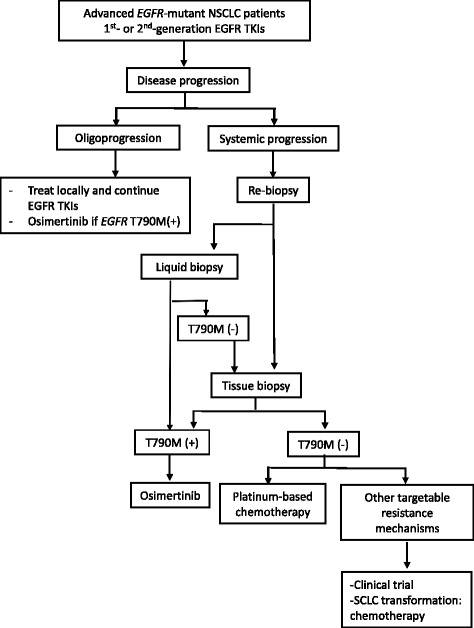
Recent advances in diagnosis and treatment are enabling a more targeted approach to treating lung cancers. Therapy targeting the specific oncogenic driver mutation could inhibit tumor progression and provide a favorable prognosis in clinical practice. Activating mutations of epidermal growth factor receptor (EGFR) in non-small cell lung cancer (NSCLC) are a favorable predictive factor for EGFR tyrosine kinase inhibitors (TKIs) treatment. For lung cancer patients with EGFR-exon 19 deletions or an exon 21 Leu858Arg mutation, the standard first-line treatment is first-generation (gefitinib, erlotinib), or second-generation (afatinib) TKIs. EGFR TKIs improve response rates, time to progression, and overall survival. Unfortunately, patients with EGFR mutant lung cancer develop disease progression after a median of 10 to 14 months on EGFR TKI. Different mechanisms of acquired resistance to first-generation and second-generation EGFR TKIs have been reported. Optimal treatment for the various mechanisms of acquired resistance is not yet clearly defined, except for the T790M mutation. Repeated tissue biopsy is important to explore resistance mechanisms, but it has limitations and risks. Liquid biopsy is a valid alternative to tissue re-biopsy. Osimertinib has been approved for patients with T790M-positive NSCLC with acquired resistance to EGFR TKI. For other TKI-resistant mechanisms, combination therapy may be considered. In addition, the use of immunotherapy in lung cancer treatment has evolved rapidly. Understanding and clarifying the biology of the resistance mechanisms of EGFR-mutant NSCLC could guide future drug development, leading to more precise therapy and advances in treatment.
近年来,诊断和治疗方面的进展使我们能够更有针对性地治疗肺癌。针对特定致癌驱动突变的治疗方法可以抑制肿瘤进展,并在临床实践中提供良好的预后。非小细胞肺癌 (NSCLC) 中表皮生长因子受体 (EGFR) 的激活突变是 EGFR 酪氨酸激酶抑制剂 (TKI) 治疗的有利预测因素。对于 EGFR 外显子 19 缺失或外显子 21 Leu858Arg 突变的肺癌患者,标准一线治疗是第一代 (吉非替尼、厄洛替尼) 或第二代 (阿法替尼) TKI。EGFR TKI 提高了反应率、进展时间和总生存期。不幸的是,EGFR 突变型肺癌患者在接受 EGFR TKI 治疗后中位 10-14 个月会出现疾病进展。已经报道了针对第一代和第二代 EGFR TKI 的获得性耐药的不同机制。除 T790M 突变外,针对各种获得性耐药机制的最佳治疗方法尚未明确。重复组织活检对于探索耐药机制很重要,但它存在局限性和风险。液体活检是组织再活检的有效替代方法。奥希替尼已被批准用于 EGFR TKI 获得性耐药的 T790M 阳性 NSCLC 患者。对于其他 TKI 耐药机制,可以考虑联合治疗。此外,免疫疗法在肺癌治疗中的应用也迅速发展。了解和阐明 EGFR 突变型 NSCLC 的耐药机制生物学特性,可以指导未来的药物开发,从而实现更精确的治疗和治疗进展。