Kim Hansoo, Comey Samantha, Hausler Karl, Cook Greg
Bristol-Myers Squib, Level 2/4 Nexus Court, Mulgrave, VIC 3170 Australia.
J Pharm Policy Pract. 2018 Feb 13;11:4. doi: 10.1186/s40545-018-0131-4. eCollection 2018.
Australian Government subsidisation of ipilimumab for the treatment of patients with metastatic melanoma was conditional on the sponsor entering a 'managed entry scheme' to assess the 2-year overall survival rate in metastatic melanoma patients who received ipilimumab in the first year of Pharmaceutical Benefits Scheme listing.
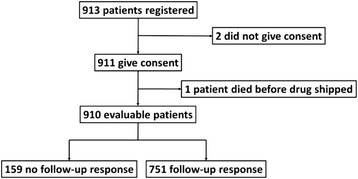
All unresectable stage IIIc / IV metastatic melanoma patients treated with at least one dose of ipilimumab therapy in Australia from the PBS listing date to a time point 12 months later (i.e. from 1-Aug-2013 to 31-Jul-2014) were invited to participate. Overall survival at 2 years post treatment initiation was measured, with Cox regression analysis used to examine the relationship between survival and patient baseline characteristics.
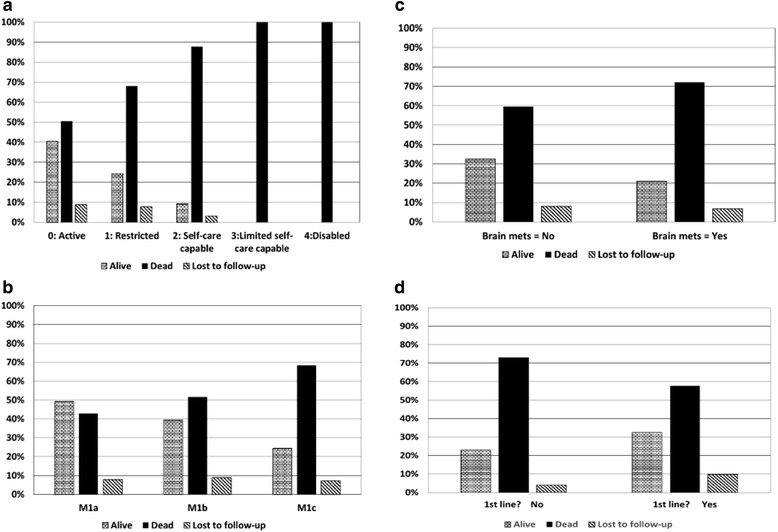
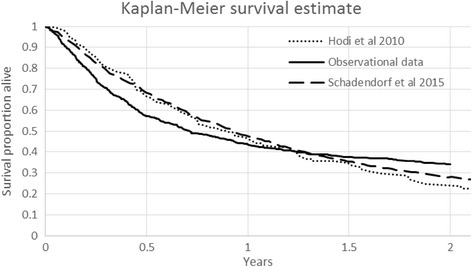
The evaluable population (910 patients) was on average 63.3 years old, male (70.1%) and treated in a public hospital (64.4%) in an urban area (76.5%). The majority of patients were treatment naïve (63.3%), did not have brain metastases (71.1%), and were classified as ECOG performance status 0 or 1 (90.4%). The 2 year overall survival rate was conservatively calculated to be at least 23.9% and potentially as high as 34.2%. A significant difference in overall survival at 2 years was demonstrated across the categories of ECOG performance status ( < 0.0001), M-status ( = 0.0005) and treatment status ( = 0.0114). No statistical difference in survival rate was observed when examining brain metastases vs no brain metastases ( = 0.2622), treatment at private vs public hospitals ( = 0.7601) nor treatment in the urban vs rural setting ( = 0.5048).
The 2 year overall survival rate for all patients receiving PBS subsidised ipilimumab in Australia from the first year Pharmaceutical Benefits Scheme cohort is estimated to be between 23.9% and 34.2%, which is higher than the 23.5% observed in the key ipilimumab registrational trial. Results and learnings from the ipilimumab 'managed entry scheme' illustrate that early access with the promise of future evidence to confirm a medicine's cost-effectiveness can work, but needs to be carefully considered, constructed and managed.
澳大利亚政府对用于治疗转移性黑色素瘤患者的伊匹木单抗进行补贴的条件是,申办方要进入“管理式进入计划”,以评估在药品福利计划(PBS)上市第一年接受伊匹木单抗治疗的转移性黑色素瘤患者的2年总生存率。
邀请了从PBS上市日期至12个月后的某个时间点(即从2013年8月1日至2014年7月31日)在澳大利亚接受至少一剂伊匹木单抗治疗的所有不可切除的IIIc期/IV期转移性黑色素瘤患者参与。测量治疗开始后2年的总生存率,采用Cox回归分析来检验生存率与患者基线特征之间的关系。
可评估人群(910例患者)的平均年龄为63.3岁,男性(70.1%),在城市地区的公立医院接受治疗(64.4%)。大多数患者未曾接受过治疗(63.3%),没有脑转移(71.1%),且被分类为东部肿瘤协作组(ECOG)体能状态为0或1(90.4%)。2年总生存率保守计算至少为23.9%,可能高达34.2%。在ECOG体能状态类别(<0.0001)、M状态(=0.0005)和治疗状态(=0.0114)中,2年总生存率存在显著差异。在检查有无脑转移(=0.2622)、私立医院与公立医院的治疗情况(=0.7601)以及城市与农村地区的治疗情况(=0.5048)时,未观察到生存率的统计学差异。
从药品福利计划队列的第一年起,在澳大利亚接受PBS补贴的伊匹木单抗治疗的所有患者的2年总生存率估计在23.9%至34.2%之间,高于伊匹木单抗关键注册试验中观察到的23.5%。伊匹木单抗“管理式进入计划”的结果和经验表明,在有未来证据有望确认药物成本效益的情况下尽早使用药物是可行的,但需要仔细考虑、构建和管理。