Tohya Akina, Kohjitani Atsushi, Ohno Sachi, Yamashita Kaoru, Manabe Yozo, Sugimura Mitsutaka
Department of Dental Anesthesiology, Field of Oral and Maxillofacial Rehabilitation, Graduate School of Medical and Dental Sciences, Kagoshima University, 8-35-1 Sakuragaoka, Kagoshima, 890-8544, Japan.
JA Clin Rep. 2018;4(1):9. doi: 10.1186/s40981-018-0148-3. Epub 2018 Jan 22.
Secretion of hormones, which antagonize the action of insulin, is facilitated in response to surgery, and acute resistance to the action of insulin develops. Our aim is to elucidate the effects of intraoperative glycemic control by glucose-insulin (GI) infusion on postoperative complications and outcomes in major oral and maxillofacial surgery.
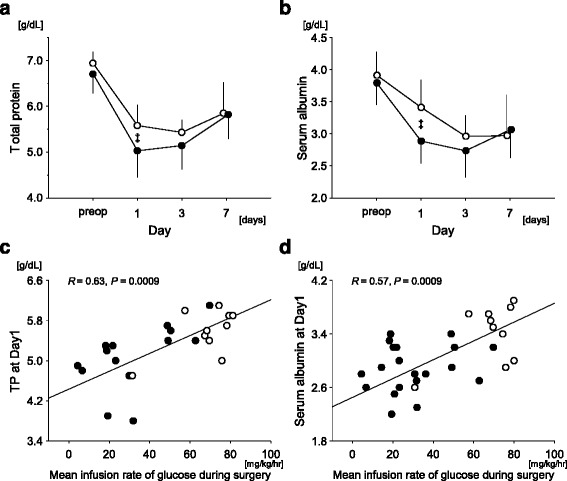
Thirty patients aged ≥ 60 years undergoing a radical operation of oral malignant tumors with tissue reconstruction (≥ 8 h) were analyzed. In the GI group, regular insulin was continuously applied with glucose-added acetate Ringer's solution (5-10 g glucose per 500 mL). Blood glucose was adjusted within the target concentration of 80-120 mg/dL. In the control group, combination of acetate Ringer's solution containing 1% (/) glucose and lactate Ringer's solution, which contains no glucose, was employed. Perioperative clinical parameters, incidence of hypoalbuminemia, and postoperative complications, i.e., surgical site infection, necrosis of a reconstructed flap, bacteremia, hypotension, or pneumonia, were compared. Both serum total protein and albumin concentrations (postoperative day 1 [Day1]) were higher in the GI group. The mean infusion rate of glucose during surgery (mg/kg/h) was independently associated with the decrease in both serum total protein and albumin concentrations from the control to Day1. No difference was found between the groups in the incidence of postoperative complications and the days required until discharge, except less incidence of hypoalbuminemia in the GI group.
Application of additional glucose during major oral and maxillofacial surgery preserved serum albumin concentration. However, it did not lead to less postoperative complications and less days until discharge.
手术可促使拮抗胰岛素作用的激素分泌,进而产生急性胰岛素抵抗。我们的目的是阐明术中葡萄糖 - 胰岛素(GI)输注控制血糖对口腔颌面外科大手术术后并发症及预后的影响。
分析了30例年龄≥60岁、接受口腔恶性肿瘤根治术并组织重建(≥8小时)的患者。在GI组中,将正规胰岛素与加葡萄糖的醋酸林格液(每500 mL含5 - 10 g葡萄糖)持续输注。血糖调整至目标浓度80 - 120 mg/dL。对照组采用含1%(/)葡萄糖的醋酸林格液和不含葡萄糖的乳酸林格液联合使用。比较围手术期临床参数、低蛋白血症发生率及术后并发症,即手术部位感染、重建皮瓣坏死、菌血症、低血压或肺炎。GI组术后第1天(Day1)的血清总蛋白和白蛋白浓度均较高。手术期间葡萄糖的平均输注速率(mg/kg/h)与从对照组到Day1血清总蛋白和白蛋白浓度的降低独立相关。除GI组低蛋白血症发生率较低外,两组术后并发症发生率和出院所需天数无差异。
口腔颌面外科大手术期间额外补充葡萄糖可维持血清白蛋白浓度。然而,这并未减少术后并发症及缩短出院天数。