Department of Pathology, The University of Texas MD Anderson Cancer Center, Houston, Texas.
Department of Dermatologic Oncology, National Cancer Center Hospital, Tokyo, Japan.
Cancer Med. 2018 Mar;7(3):583-593. doi: 10.1002/cam4.1320. Epub 2018 Feb 21.
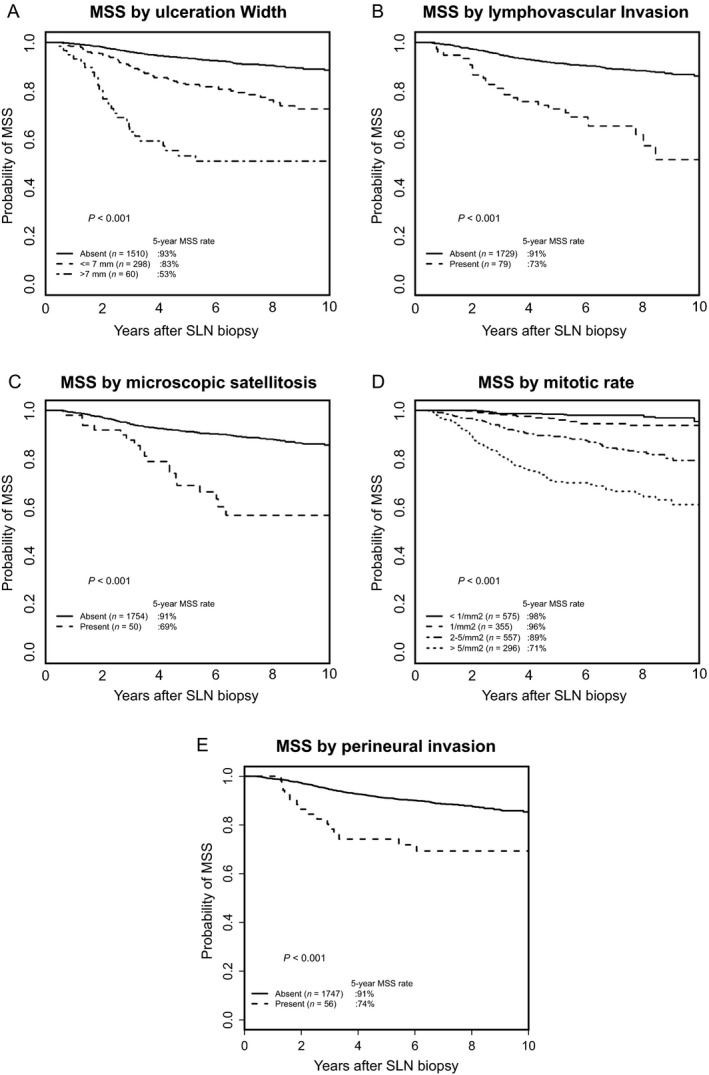
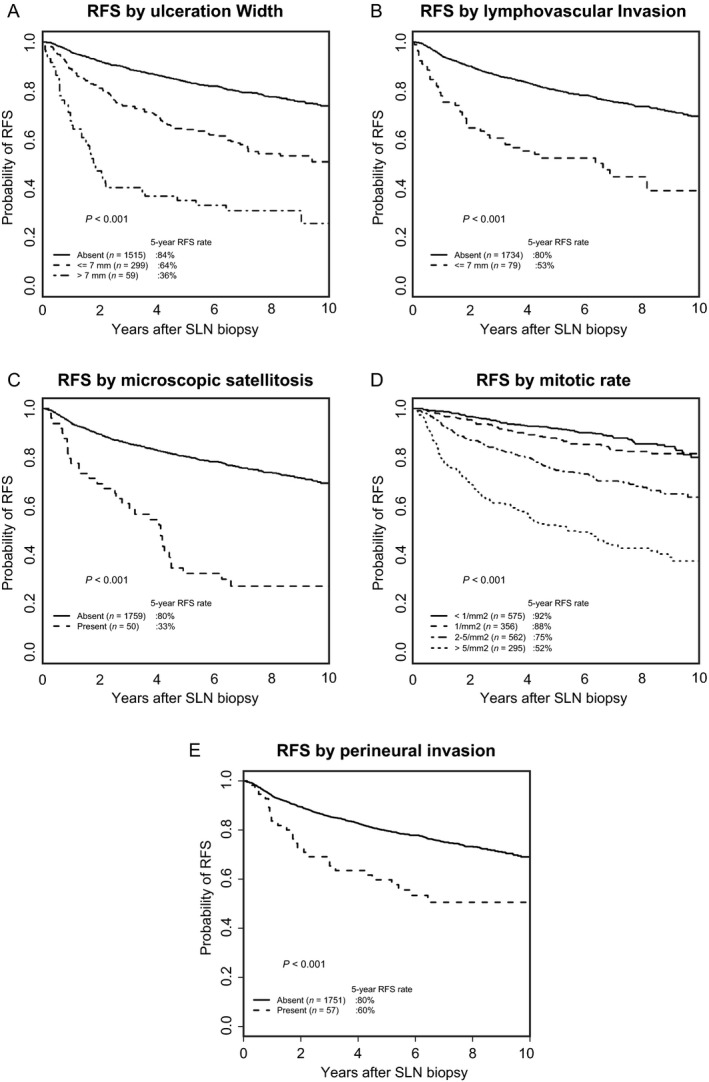
The prognostic significance of the width of the ulceration in primary melanomas remains unclear, and there is a relative paucity of data for lymphovascular invasion (LVI), microscopic satellitosis (MS), perineural invasion (PNI), and mitotic rate when compared with other pathological elements currently required for reporting. To evaluate the prognostic importance of the ulceration width and other important pathologic measurements, a single-institutional retrospective study was conducted using records of cutaneous melanoma patients who underwent sentinel lymph node (SLN) biopsy at The University of Texas, MD Anderson Cancer Center between 2003 and 2008. We identified 1898 eligible patients with median tumor thickness of 1.25 mm and median follow-up of 6.7 years. By multivariable analyses, the strongest risk factor for SLN positivity was high tumor thickness followed by the presence of LVI. The pathologic measures with the strongest influence on recurrence-free survival (RFS) were tumor thickness and positive SLN status. Ulceration width and presence of MS were also significantly associated with RFS while PNI was not. Factors with the strongest influence on melanoma-specific survival (MSS) were positive SLN status and mitotic rate. In conclusion, SLN biopsy should probably be offered if the primary tumor has LVI. MS is an adverse prognostic factor for RFS, but its influence on outcome is modest. Ulceration width predicts RFS but loses its independent prognostic significance for MSS when adjusting for currently used clinicopathological factors. In view of its impact on MSS, mitotic rate should be recorded for cutaneous invasive melanomas across all T categories.
原发性黑色素瘤的溃疡宽度的预后意义尚不清楚,与目前报告所需的其他病理元素相比,其淋巴血管侵犯(LVI)、微观卫星病(MS)、神经周围侵犯(PNI)和有丝分裂率的数据相对较少。为了评估溃疡宽度和其他重要病理测量的预后重要性,使用 2003 年至 2008 年间在德克萨斯大学 MD 安德森癌症中心接受前哨淋巴结(SLN)活检的皮肤黑色素瘤患者的记录,进行了单机构回顾性研究。我们确定了 1898 名符合条件的患者,其肿瘤厚度中位数为 1.25mm,中位随访时间为 6.7 年。通过多变量分析,SLN 阳性的最强危险因素是高肿瘤厚度,其次是 LVI 的存在。对无复发生存(RFS)影响最大的病理测量是肿瘤厚度和 SLN 阳性状态。溃疡宽度和 MS 的存在与 RFS 显著相关,而 PNI 则没有。对黑色素瘤特异性生存(MSS)影响最大的因素是 SLN 阳性状态和有丝分裂率。总之,如果原发性肿瘤存在 LVI,则可能需要进行 SLN 活检。MS 是 RFS 的不良预后因素,但对结局的影响不大。溃疡宽度预测 RFS,但在调整当前使用的临床病理因素后,其对 MSS 的独立预后意义丧失。鉴于其对 MSS 的影响,应记录所有 T 分期的皮肤浸润性黑色素瘤的有丝分裂率。