Department of Breast Surgery, The First Affiliated Hospital of Chongqing Medical University, No.1 Youyi Road, Yuzhong District, Chongqing, 400042, China.
Breast Cancer Res Treat. 2018 Jul;170(1):35-43. doi: 10.1007/s10549-018-4730-1. Epub 2018 Feb 26.
To assess the predictive role of pretreatment ki67 and Ki67 changes in breast cancer (BC) patients treated with neoadjuvant chemotherapy (NAC) in various molecular subtypes.
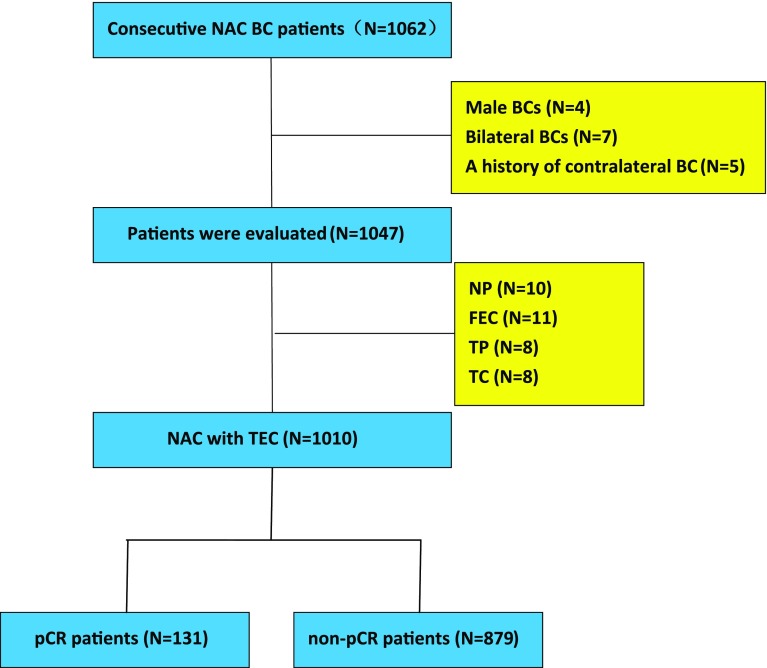
1010 BC patients who had undergone anthracycline and taxane-based NAC from January 2012 to July 2017 were retrospectively analyzed. Clinical and pathological parameters of the patients were retrieved and the predictive factors for NAC response were evaluated.
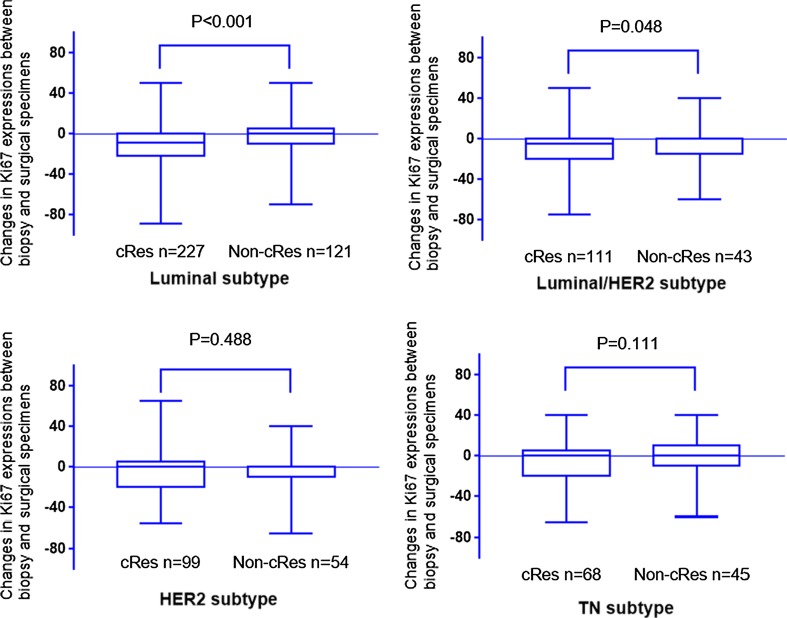
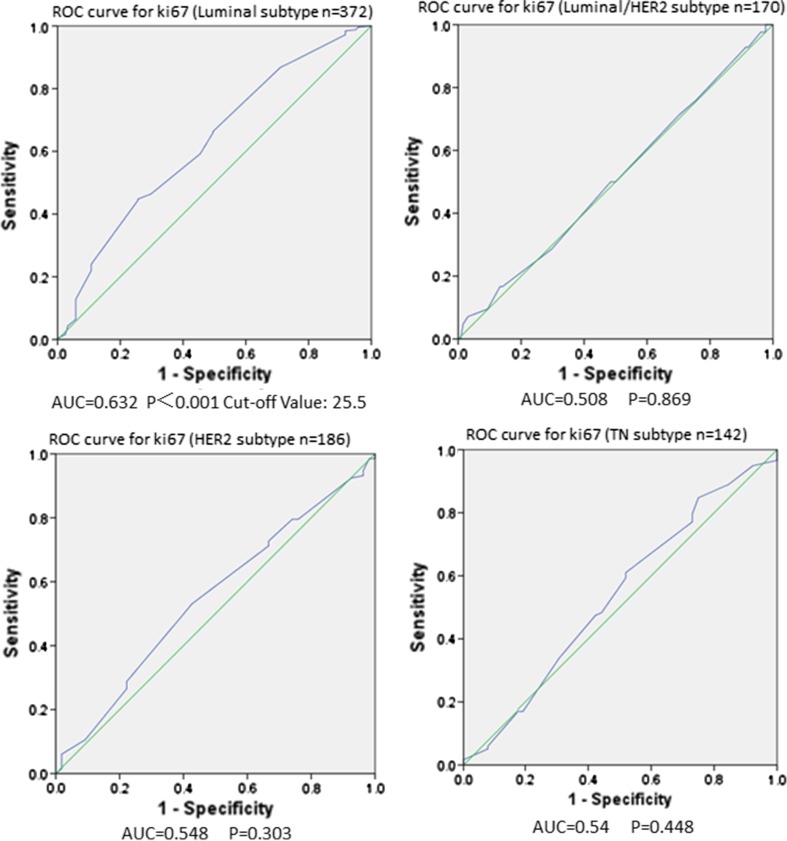
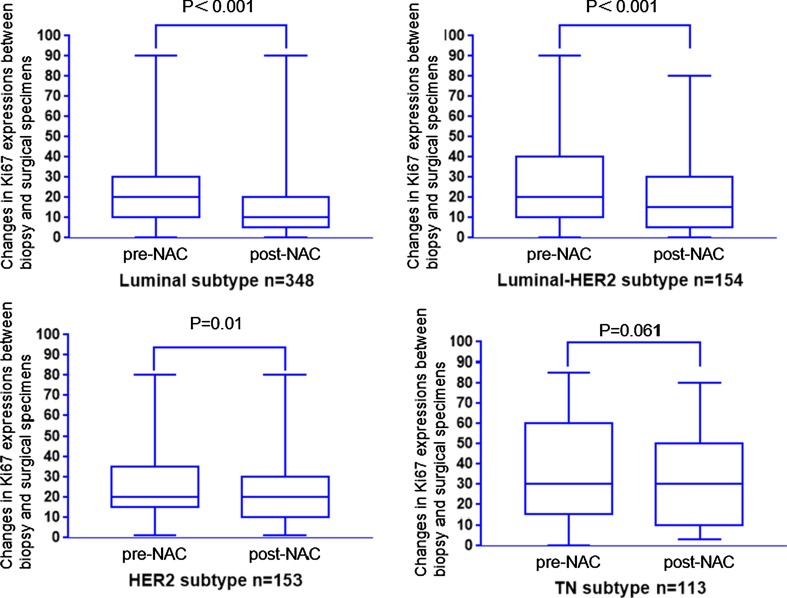
705 patients showed clinical response (cRes), and 131 patients acquired pathologic complete response (pCR). Patients with higher pretreatment Ki67 (≥ 14%), tumor size ≥ 4 cm, and positive clinical nodal had better clinical therapy response, while patients with negative ER and PR, higher pretreatment Ki67 (≥ 14%), and tumor size < 4 cm were more probable to attain pCR. The pretreatment Ki67 could be used as a predictor of NAC only in luminal subtypes, and 25.5% were identified as an ideal cut-off point to differentiate the cRes from non-cRes cases. Although a decrease in Ki67 had been found in almost all molecular subtypes after NAC, no statistically significant differences were found in the decrease of Ki67 were validated between the cRes and non-cRes group in HER2-rich and triple-negative subtypes (P = 0.488 and P = 0.111, respectively).
The best cut-off for pretreatment Ki67 in predicting the connection with the tumor size lessening was 25.5% in luminal subtype. Aggressive adjuvant systemic treatments should be considered for patients with HER2-rich and triple-negative subtype who exhibit tumor shrinkage in NAC but still have high levels of Ki67.
评估新辅助化疗(NAC)治疗的乳腺癌(BC)患者治疗前 Ki67 和 Ki67 变化在各种分子亚型中的预测作用。
回顾性分析 2012 年 1 月至 2017 年 7 月期间接受蒽环类和紫杉烷类 NAC 的 1010 例 BC 患者。检索患者的临床和病理参数,并评估 NAC 反应的预测因素。
705 例患者表现出临床缓解(cRes),131 例患者获得病理完全缓解(pCR)。Ki67 水平较高(≥14%)、肿瘤大小≥4cm 和阳性临床淋巴结的患者具有更好的临床治疗反应,而 ER 和 PR 阴性、Ki67 水平较高(≥14%)和肿瘤大小<4cm 的患者更有可能获得 pCR。治疗前 Ki67 可作为 NAC 的预测因子,但仅在管腔亚型中有用,25.5%被确定为区分 cRes 和非 cRes 病例的理想临界点。尽管在 NAC 后几乎所有分子亚型的 Ki67 都有所下降,但在 HER2 丰富型和三阴性亚型中,cRes 组和非 cRes 组之间 Ki67 下降的差异无统计学意义(P=0.488 和 P=0.111)。
在管腔亚型中,预测肿瘤大小缩小与 Ki67 相关性的最佳预处理 Ki67 截止值为 25.5%。对于在 NAC 中显示肿瘤缩小但 Ki67 水平仍然较高的 HER2 丰富型和三阴性亚型患者,应考虑进行强化辅助全身治疗。