Russo Raffaele, Maiotti Marco, Taverna Ettore
Orthopedics and Traumatology Unit, Pellegrini Hospital, Via Portamedina alla Pignasecca 41, 80134, Naples, Italy.
Sports Medicine Unit & Orthopedic Center, San Giovanni Addolorata Hospital, Via dell'Amba Aradam 9, 00184, Rome, Italy.
J Exp Orthop. 2018 Feb 27;5(1):5. doi: 10.1186/s40634-018-0121-0.
Glenoid bone loss and capsular deficiency represent critical points of arthroscopic Bankart repair failures. The purpose of this study was to evaluate an all-arthroscopic bone block procedure associated with arthroscopic subscapularis augmentation (ASA) for treating gleno-humeral instability with glenoid bone loss (GBL) and anterior capsulo-labral deficiency. Our hypothesis was that these two procedures could be combined arthroscopically. The feasibility of this technique and its reproducibility, and potential neurovascular complications were evaluated.
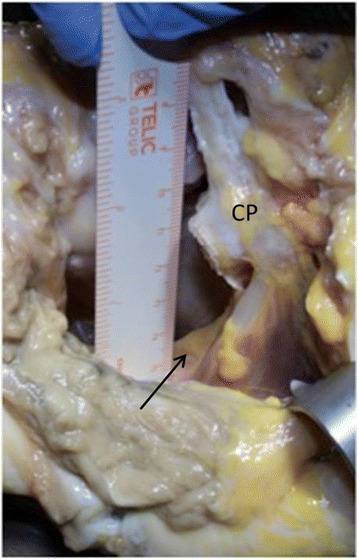
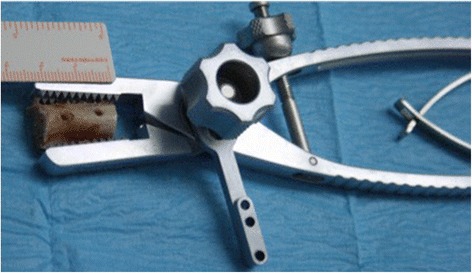
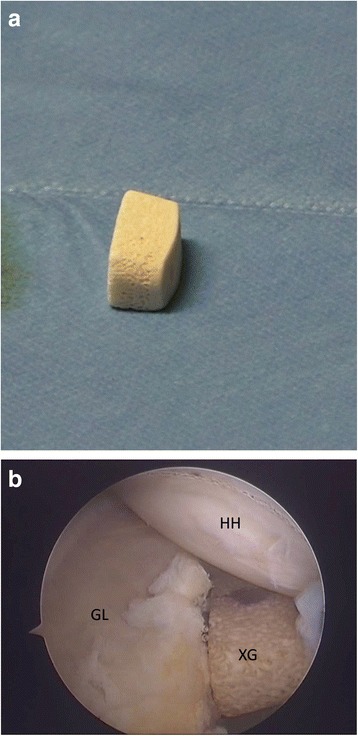
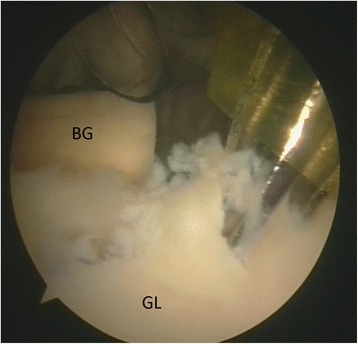
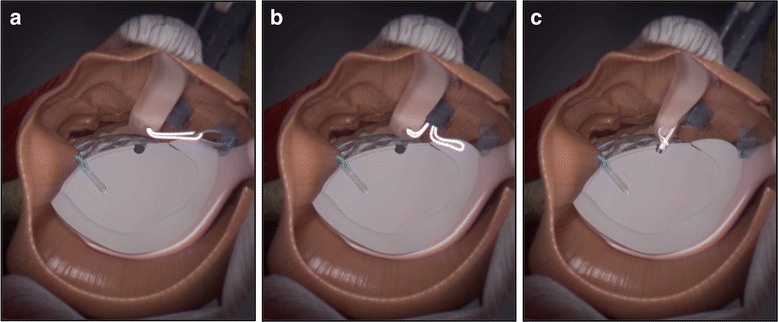
A tricortical bone graft was harvested from the cadaveric clavicle, and in one case a Xenograft was used. An anterior-inferior GBL of about 25% was created. Two glenoid tunnels were set up from the posterior to the anterior side using a dedicated bone block guide, and four buttons were used to fix the graft to the glenoid. The subscapularis tenodesis was performed using a suture tape anchor. Afterwards, the shoulder was dissected to study the relationship between all portals and nerves. The size of the bone block, its position on the glenoid and the relationship with the subscapularis tendon were investigated.
In all seven specimens (five left and two right shoulders), the bone block was flush with the cartilage and fixed to the anterior-inferior part of the glenoid. No lesions of the surrounding neurovascular structures were observed. No interference was found between the two bone block tunnels and the anchor tunnel used for the tenodesis.
This study demonstrated the feasibility and reproducibility of this combined arthroscopic technique (bone block associated with ASA) in the treatment of anterior shoulder instability associated with anterior bone loss and anterior capsular deficiency.
肩胛盂骨丢失和关节囊缺损是关节镜下Bankart修复失败的关键点。本研究的目的是评估一种与关节镜下肩胛下肌增强术(ASA)相关的全关节镜骨块手术,用于治疗伴有肩胛盂骨丢失(GBL)和前关节盂唇韧带缺损的肩肱关节不稳。我们的假设是这两种手术可以在关节镜下联合进行。评估了该技术的可行性、可重复性以及潜在的神经血管并发症。
从尸体锁骨获取一块三层皮质骨移植骨,在1例中使用了异种移植骨。制造了约25%的前下GBL。使用专用骨块导向器从前向后建立两个肩胛盂隧道,并用4个纽扣将移植骨固定到肩胛盂上。使用缝线带锚钉进行肩胛下肌固定术。之后,解剖肩部以研究所有入路与神经之间的关系。研究了骨块的大小、其在肩胛盂上的位置以及与肩胛下肌腱的关系。
在所有7个标本(5个左肩和2个右肩)中,骨块与软骨齐平并固定在肩胛盂的前下部。未观察到周围神经血管结构的损伤。在两个骨块隧道与用于固定术的锚钉隧道之间未发现干扰。
本研究证明了这种联合关节镜技术(骨块联合ASA)在治疗伴有前部骨丢失和前关节囊缺损的前肩不稳方面的可行性和可重复性。