Oxford Centre for Clinical Magnetic Resonance Research, Division of Cardiovascular Medicine, Radcliffe Department of Medicine, University of Oxford, Oxford, United Kingdom.
Oxford Heart Centre, John Radcliffe Hospital, Oxford, United Kingdom.
J Am Coll Cardiol. 2018 Mar 6;71(9):969-979. doi: 10.1016/j.jacc.2017.12.046.
In patients with angina and nonobstructive coronary artery disease (NOCAD), confirming symptoms due to coronary microvascular dysfunction (CMD) remains challenging. Cardiac magnetic resonance (CMR) assesses myocardial perfusion with high spatial resolution and is widely used for diagnosing obstructive coronary artery disease (CAD).
The goal of this study was to validate CMR for diagnosing microvascular angina in patients with NOCAD, compared with patients with obstructive CAD and correlated to the index of microcirculatory resistance (IMR) during invasive coronary angiography.
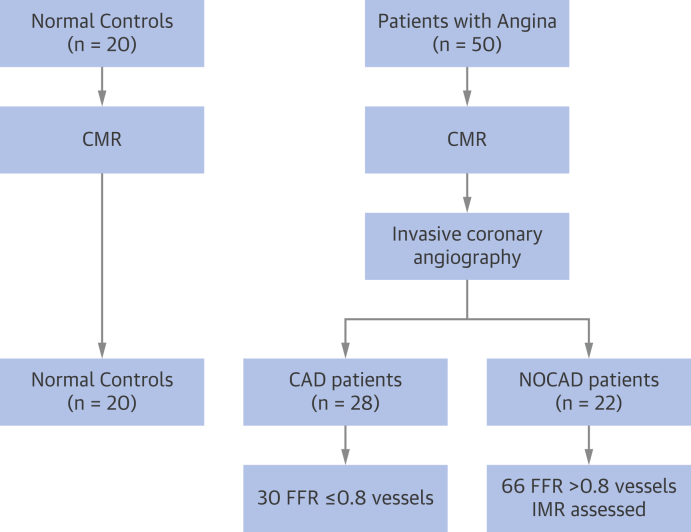
Fifty patients with angina (65 ± 9 years of age) and 20 age-matched healthy control subjects underwent adenosine stress CMR (1.5- and 3-T) to assess left ventricular function, inducible ischemia (myocardial perfusion reserve index [MPRI]; myocardial blood flow [MBF]), and infarction (late gadolinium enhancement). During subsequent angiography within 7 days, 28 patients had obstructive CAD (fractional flow reserve [FFR] ≤0.8) and 22 patients had NOCAD (FFR >0.8) who underwent 3-vessel IMR measurements.
In patients with NOCAD, myocardium with IMR <25 U had normal MPRI (1.9 ± 0.4 vs. controls 2.0 ± 0.3; p = 0.49); myocardium with IMR ≥25 U had significantly impaired MPRI, similar to ischemic myocardium downstream of obstructive CAD (1.2 ± 0.3 vs. 1.2 ± 0.4; p = 0.61). An MPRI of 1.4 accurately detected impaired perfusion related to CMD (IMR ≥25 U; FFR >0.8) (area under the curve: 0.90; specificity: 95%; sensitivity: 89%; p < 0.001). Impaired MPRI in patients with NOCAD was driven by impaired augmentation of MBF during stress, with normal resting MBF. Myocardium with FFR >0.8 and normal IMR (<25 U) still had blunted stress MBF, suggesting mild CMD, which was distinguishable from control subjects by using a stress MBF threshold of 2.3 ml/min/g with 100% positive predictive value.
In angina patients with NOCAD, CMR can objectively and noninvasively assess microvascular angina. A CMR-based combined diagnostic pathway for both epicardial and microvascular CAD deserves further clinical validation.
在有胸痛和非阻塞性冠状动脉疾病(NOCAD)的患者中,证实由冠状动脉微血管功能障碍(CMD)引起的症状仍然具有挑战性。心脏磁共振(CMR)具有高空间分辨率,可用于评估心肌灌注,广泛用于诊断阻塞性冠状动脉疾病(CAD)。
本研究的目的是通过与阻塞性 CAD 患者和与冠状动脉造影期间的微血管阻力指数(IMR)相关联的患者进行比较,验证 CMR 诊断 NOCAD 患者微血管性心绞痛的能力。
50 名有胸痛(65±9 岁)的患者和 20 名年龄匹配的健康对照者接受腺苷负荷 CMR(1.5 和 3T)检查,以评估左心室功能、可诱导的缺血(心肌灌注储备指数[MPRI];心肌血流[MBF])和梗死(晚期钆增强)。在 7 天内进行的后续血管造影期间,28 名患者有阻塞性 CAD(血流储备分数[FFR]≤0.8),22 名患者有 NOCAD(FFR>0.8),他们接受了 3 支血管 IMR 测量。
在 NOCAD 患者中,IMR<25 U 的心肌有正常的 MPRI(1.9±0.4 比对照组 2.0±0.3;p=0.49);IMR≥25 U 的心肌有明显的 MPRI 受损,类似于阻塞性 CAD 下游的缺血性心肌(1.2±0.3 比 1.2±0.4;p=0.61)。MPRI 为 1.4 可以准确检测到与 CMD 相关的灌注受损(IMR≥25 U;FFR>0.8)(曲线下面积:0.90;特异性:95%;敏感性:89%;p<0.001)。NOCAD 患者中 MPRI 受损是由应激时 MBF 增加受损引起的,静息时 MBF 正常。FFR>0.8 和 IMR 正常(<25 U)的心肌仍有应激时 MBF 迟钝,提示存在轻度 CMD,这可以通过使用 100%阳性预测值的 2.3ml/min/g 的应激 MBF 阈值与对照组区分开来。
在有 NOCAD 的胸痛患者中,CMR 可以客观、无创地评估微血管性心绞痛。基于 CMR 的诊断方法,包括心外膜和微血管 CAD,值得进一步的临床验证。