Kerwat Doa'a, Zargaran Alexander, Bharamgoudar Reshma, Arif Nadia, Bello Grace, Sharma Bharat, Kerwat Rajab
Department of Medicine, Barts and The London.
Department of Medicine, St George's University of London, London.
Clinicoecon Outcomes Res. 2018 Feb 19;10:119-125. doi: 10.2147/CEOR.S149924. eCollection 2018.
This economic evaluation quantifies the cost-effectiveness of early laparoscopic cholecystectomy (ELC) versus delayed laparoscopic cholecystectomy (DLC) in the management of acute cholecystitis. The two interventions were assessed in terms of outcome measures, including utilities, to derive quality-adjusted life years (QALYs) as a unit of effectiveness. This study hypothesizes that ELC is more cost-effective than DLC.
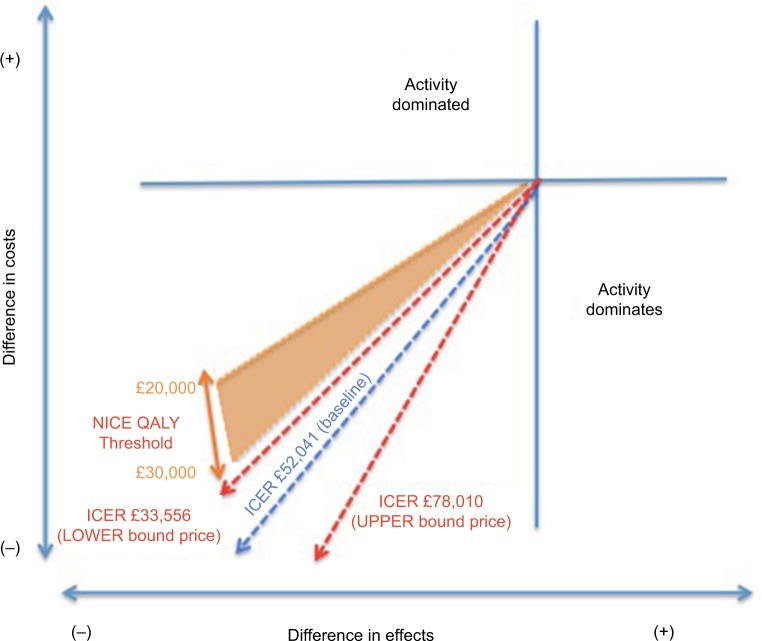
In this economic evaluation, existing literature was compiled and analyzed to estimate the incremental cost-effectiveness of ELC versus DLC. Six randomized controlled trials were used to schematically represent the probabilities of each decision tree branch. To calculate health outcomes, quality of life scores were sourced from three articles and multiplied by the expected length of life postintervention to give QALYs. From an National Health Service (NHS) perspective, one QALY may be sacrificed if the incremental cost-effectiveness ratio is above £20,000-£30,0000 in cost savings.
This economic evaluation calculated the average net present values of ELC to be £3920 and DLC to be £4565, demonstrating that ELC is the less-expensive intervention, with potential cost savings of £645 per operation. When scaling these savings up to a population approximately comparable to the size of the UK, full-scale implementation of ELC rather than DLC will potentially save the NHS £30,000,000 per annum.
ELCs are cost-effective from the perspective of the NHS. As such, policy should review existing guidelines and consider the merits of ELC versus DLC, improving resource allocation. The findings of this article advocate that ELC should become a standard practice.
本经济评估量化了早期腹腔镜胆囊切除术(ELC)与延迟腹腔镜胆囊切除术(DLC)在急性胆囊炎治疗中的成本效益。从包括效用在内的结局指标方面对这两种干预措施进行评估,以得出质量调整生命年(QALYs)作为有效性单位。本研究假设ELC比DLC更具成本效益。
在本经济评估中,收集并分析现有文献以估计ELC与DLC的增量成本效益。六项随机对照试验用于示意性地表示每个决策树分支的概率。为计算健康结局,生活质量评分来自三篇文章,并乘以干预后预期寿命以得出QALYs。从英国国家医疗服务体系(NHS)的角度来看,如果增量成本效益比高于20,000 - 30,000英镑的成本节约,则可能会牺牲一个QALY。
本经济评估计算出ELC的平均净现值为3920英镑,DLC为4565英镑,表明ELC是成本较低的干预措施,每次手术潜在成本节约645英镑。将这些节约量扩大到与英国规模大致相当的人群时,全面实施ELC而非DLC每年可能为NHS节省3000万英镑。
从NHS的角度来看,ELC具有成本效益。因此,政策应审查现有指南,并考虑ELC与DLC的优缺点,改善资源分配。本文的研究结果主张ELC应成为标准做法。