Department of Urologic Surgery, Vanderbilt University Medical Center, Nashville, TN, USA; Department of Urology, Mayo Clinic Hospital, Phoenix, AZ, USA.
Department of Biostatistics, Vanderbilt University School of Medicine, Nashville, TN, USA.
Eur Urol. 2018 Jul;74(1):26-33. doi: 10.1016/j.eururo.2018.02.012. Epub 2018 Feb 28.
Whether prostate cancer severity modifies patient-reported functional outcomes after radical prostatectomy (RP) or external beam radiotherapy (EBRT) for localized cancer is unknown.
The purpose of this study was to determine whether differences in predicted function over time between RP and EBRT varied by risk group.
DESIGN, SETTING, AND PARTICIPANTS: The Comparative Effectiveness Analysis of Surgery and Radiation (CEASAR) study is a prospective, population-based, observational study that enrolled men with localized prostate cancer in 2011-2012. Among 2117 CEASAR participants who underwent RP or EBRT, 817 had low-risk, 902 intermediate-risk, and 398 high-risk disease.
Patient-reported, disease-specific function was measured using the 26-item Expanded Prostate Index Composite (at baseline and 6, 12, and 36 mo). Predicted function was estimated using regression models and compared by disease risk.
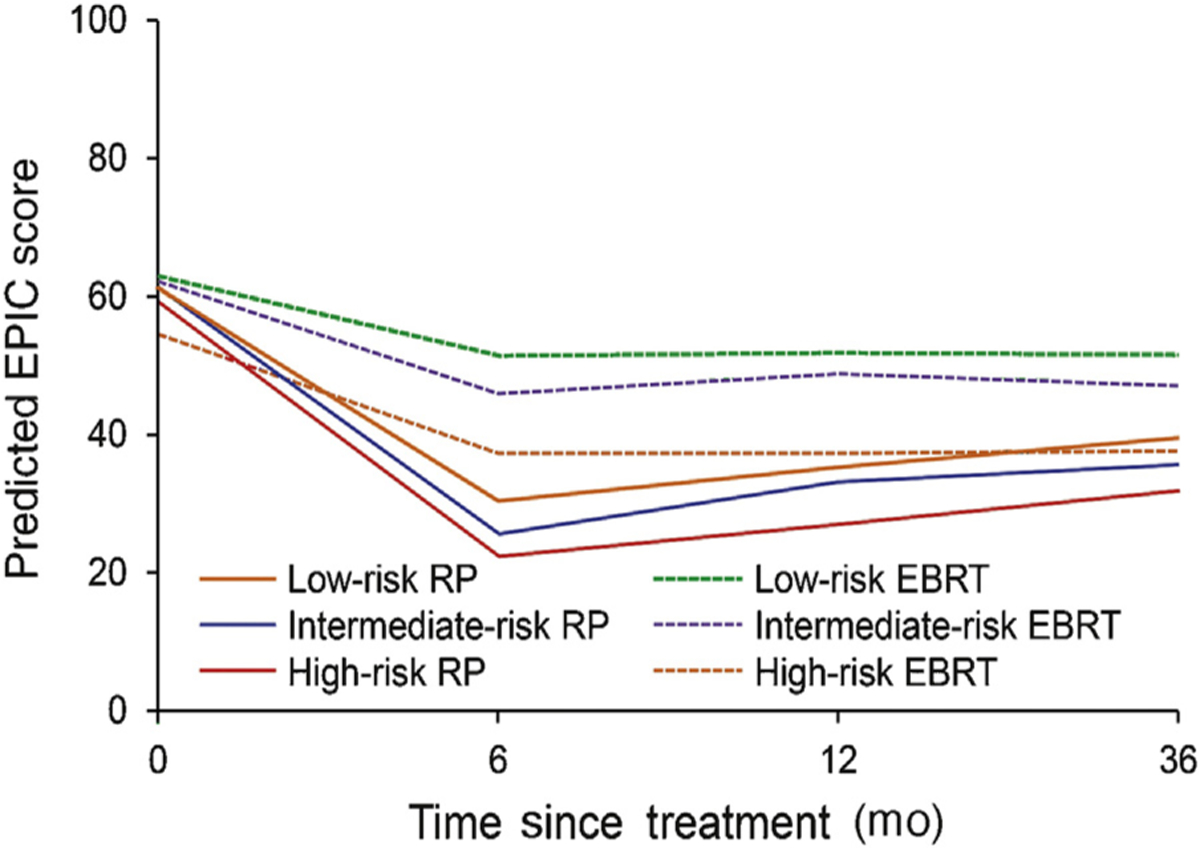
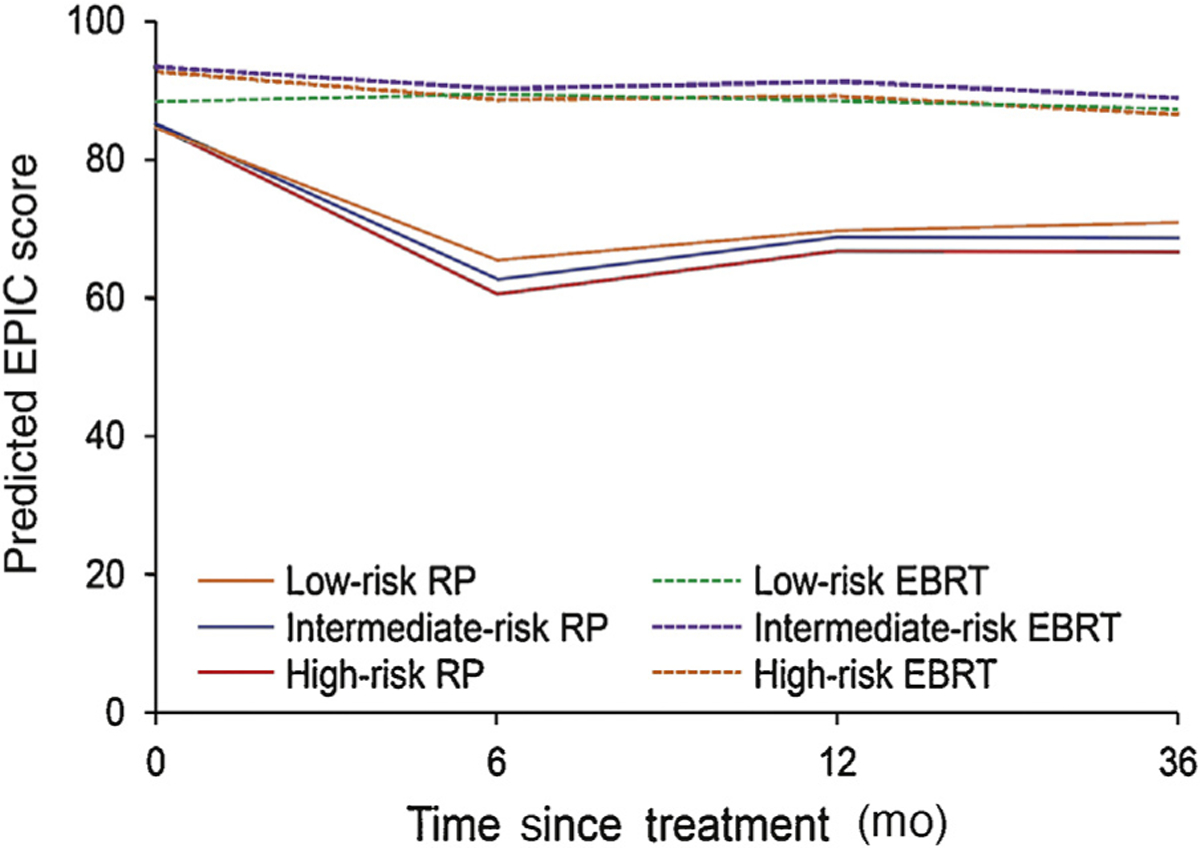
Low-risk EBRT patients reported 3-yr sexual function scores 12 points higher than those of low-risk RP patients (RP, 39 points [95% confidence interval {CI}, 37-42] vs EBRT, 52 points [95% CI, 47-56]; p<0.001). The difference in 3-yr scores for high-risk patients was not clinically significant (RP, 32 points [95% CI, 28-35] vs EBRT, 38 points [95% CI, 33-42]; p=0.03). However, when using a commonly used binary definition of sexual function (erections firm enough for intercourse), no major differences were noted between RP and EBRT at 3 yr across low-, intermediate-, and high-risk disease strata. No clinically significant interactive effects between treatment and cancer severity were observed for incontinence, bowel, irritative voiding, and hormone domains. The primary limitation is the lack of firmly established thresholds for clinically significant differences in Expanded Prostate Index Composite domain scores.
For men with low-risk prostate cancer, EBRT was associated with higher sexual function scores at 3 yr than RP; however, for men with high-risk prostate cancer, no clinically significant difference was noted. Men with high-risk prostate cancer should be counseled that EBRT and RP carry similar sexual function outcomes at 3 yr.
In this report, we studied the urinary, sexual, bowel, and hormonal functions of patients 3 yr after undergoing prostate cancer surgery or radiation. We found that for patients with high-risk disease, sexual function was similar between surgery and radiation. We conclude that high-risk patients undergoing radiation therapy should be counseled that sexual function may not be as good as low-risk patients undergoing radiation.
根治性前列腺切除术(RP)或外束放射治疗(EBRT)治疗局限性前列腺癌后,前列腺癌严重程度是否会改变患者报告的功能结局尚不清楚。
本研究旨在确定 RP 和 EBRT 之间随时间预测功能的差异是否因风险组而异。
设计、地点和参与者:比较手术和放射治疗的有效性分析(CEASAR)研究是一项前瞻性、基于人群的观察性研究,于 2011-2012 年招募了患有局限性前列腺癌的男性。在 2117 名接受 RP 或 EBRT 的 CEASAR 参与者中,817 名患有低危疾病,902 名患有中危疾病,398 名患有高危疾病。
通过 26 项扩展前列腺指数综合(在基线和 6、12 和 36 个月时)测量患者报告的疾病特异性功能。使用回归模型估计预测功能,并按疾病风险进行比较。
低危 EBRT 患者报告的 3 年性功能评分比低危 RP 患者高 12 分(RP,39 分[95%置信区间{CI},37-42] vs EBRT,52 分[95% CI,47-56];p<0.001)。高危患者的 3 年评分差异无临床意义(RP,32 分[95% CI,28-35] vs EBRT,38 分[95% CI,33-42];p=0.03)。然而,当使用性功能的常用二进制定义(勃起足以进行性交)时,在低危、中危和高危疾病各层中,在 3 年时,RP 和 EBRT 之间未观察到显著差异。未观察到治疗和癌症严重程度之间存在明显的交互作用。主要局限性在于缺乏确定扩展前列腺指数综合领域分数有临床意义差异的明确阈值。
对于患有低危前列腺癌的男性,EBRT 在 3 年内与更高的性功能评分相关;然而,对于患有高危前列腺癌的男性,没有观察到有临床意义的差异。应告知患有高危前列腺癌的男性,EBRT 和 RP 在 3 年内具有相似的性功能结局。
在本报告中,我们研究了患者接受前列腺癌手术或放疗 3 年后的尿、性、肠和激素功能。我们发现,对于高危疾病患者,手术和放疗之间的性功能相似。我们得出结论,接受放射治疗的高危患者应被告知,他们的性功能可能不如接受放射治疗的低危患者好。