MRC Epidemiology Unit, University of Cambridge, Cambridge, United Kingdom.
MRC Biostatistics Unit, University of Cambridge, Cambridge, United Kingdom.
PLoS Med. 2018 Mar 6;15(3):e1002517. doi: 10.1371/journal.pmed.1002517. eCollection 2018 Mar.
The National Health Service (NHS) Health Check programme was introduced in 2009 in England to systematically assess all adults in midlife for cardiovascular disease risk factors. However, its current benefit and impact on health inequalities are unknown. It is also unclear whether feasible changes in how it is delivered could result in increased benefits. It is one of the first such programmes in the world. We sought to estimate the health benefits and effect on inequalities of the current NHS Health Check programme and the impact of making feasible changes to its implementation.
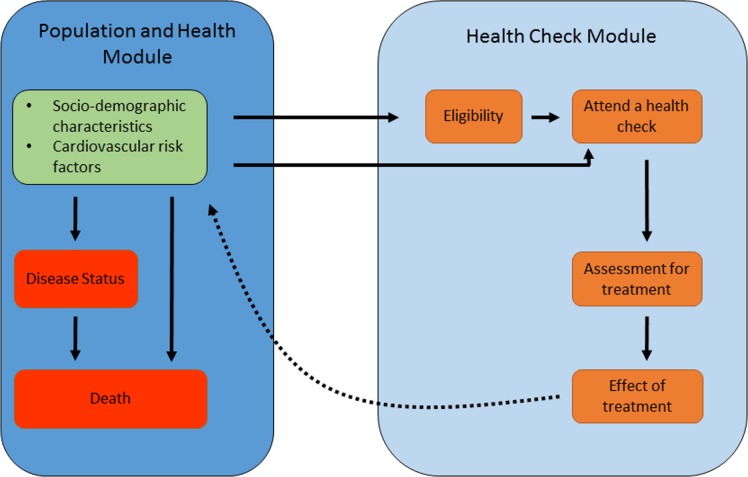
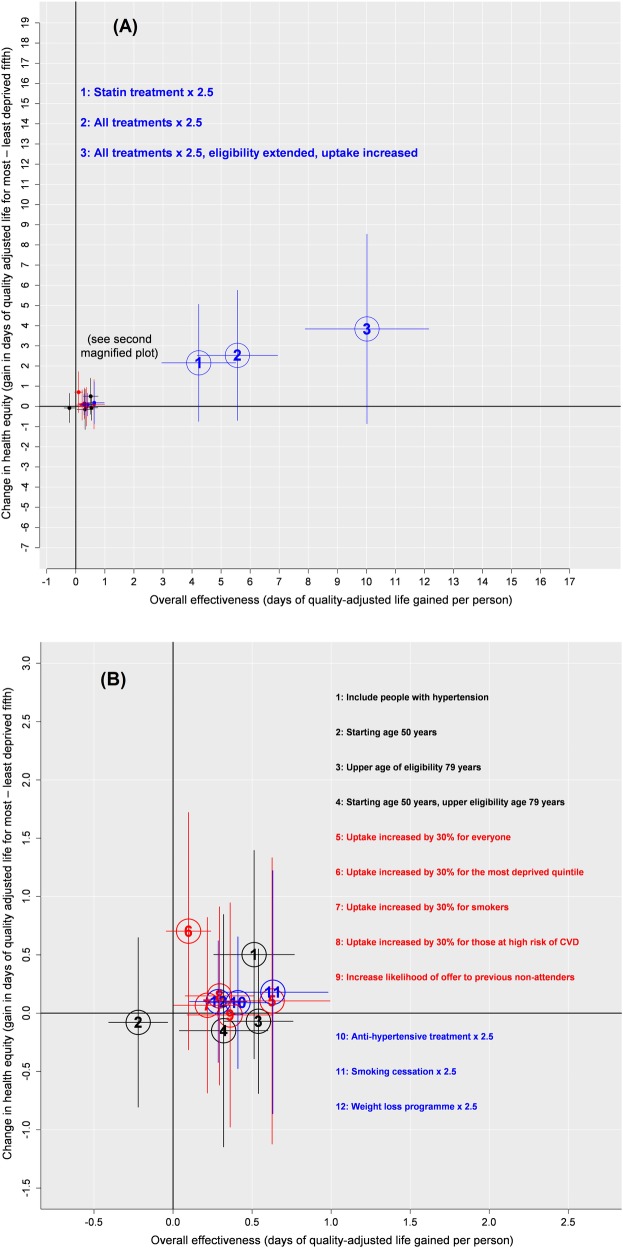
We developed a microsimulation model to estimate the health benefits (incident ischaemic heart disease, stroke, dementia, and lung cancer) of the NHS Health Check programme in England. We simulated a population of adults in England aged 40-45 years and followed until age 100 years, using data from the Health Survey of England (2009-2012) and the English Longitudinal Study of Aging (1998-2012), to simulate changes in risk factors for simulated individuals over time. We used recent programme data to describe uptake of NHS Health Checks and of 4 associated interventions (statin medication, antihypertensive medication, smoking cessation, and weight management). Estimates of treatment efficacy and adherence were based on trial data. We estimated the benefits of the current NHS Health Check programme compared to a healthcare system without systematic health checks. This counterfactual scenario models the detection and treatment of risk factors that occur within 'routine' primary care. We also explored the impact of making feasible changes to implementation of the programme concerning eligibility, uptake of NHS Health Checks, and uptake of treatments offered through the programme. We estimate that the NHS Health Check programme prevents 390 (95% credible interval 290 to 500) premature deaths before 80 years of age and results in an additional 1,370 (95% credible interval 1,100 to 1,690) people being free of disease (ischaemic heart disease, stroke, dementia, and lung cancer) at age 80 years per million people aged 40-45 years at baseline. Over the life of the cohort (i.e., followed from 40-45 years to 100 years), the changes result in an additional 10,000 (95% credible interval 8,200 to 13,000) quality-adjusted life years (QALYs) and an additional 9,000 (6,900 to 11,300) years of life. This equates to approximately 300 fewer premature deaths and 1,000 more people living free of these diseases each year in England. We estimate that the current programme is increasing QALYs by 3.8 days (95% credible interval 3.0-4.7) per head of population and increasing survival by 3.3 days (2.5-4.1) per head of population over the 60 years of follow-up. The current programme has a greater absolute impact on health for those living in the most deprived areas compared to those living in the least deprived areas (4.4 [2.7-6.5] days of additional quality-adjusted life per head of population versus 2.8 [1.7-4.0] days; 5.1 [3.4-7.1] additional days lived per head of population versus 3.3 [2.1-4.5] days). Making feasible changes to the delivery of the existing programme could result in a sizable increase in the benefit. For example, a strategy that combines extending eligibility to those with preexisting hypertension, extending the upper age of eligibility to 79 years, increasing uptake of health checks by 30%, and increasing treatment rates 2.5-fold amongst eligible patients (i.e., 'maximum potential' scenario) results in at least a 3-fold increase in benefits compared to the current programme (1,360 premature deaths versus 390; 5,100 people free of 1 of the 4 diseases versus 1,370; 37,000 additional QALYs versus 10,000; 33,000 additional years of life versus 9,000). Ensuring those who are assessed and eligible for statins receive statins is a particularly important strategy to increase benefits. Estimates of overall benefit are based on current incidence and management, and future declines in disease incidence or improvements in treatment could alter the actual benefits observed in the long run. We have focused on the cardiovascular element of the NHS Health Check programme. Some important noncardiovascular health outcomes (e.g., chronic obstructive pulmonary disease [COPD] prevention from smoking cessation and cancer prevention from weight loss) and other parts of the programme (e.g., brief interventions to reduce harmful alcohol consumption) have not been modelled.
Our model indicates that the current NHS Health Check programme is contributing to improvements in health and reducing health inequalities. Feasible changes in the organisation of the programme could result in more than a 3-fold increase in health benefits.
英国国民保健制度(NHS)健康检查计划于 2009 年在英格兰推出,旨在系统性地评估中年人群的心血管疾病风险因素。然而,目前尚不清楚该计划对健康不平等的影响及其效益。也不清楚是否可以通过改变其实施方式来增加效益。这是世界上第一个此类计划之一。我们试图评估 NHS 健康检查计划目前的效益及其对健康不平等的影响,以及实施方式改变的可行性。
我们开发了一个微观模拟模型来估计英格兰 NHS 健康检查计划的健康效益(缺血性心脏病、中风、痴呆和肺癌的发病)。我们模拟了英格兰 40-45 岁成年人的人口,并随访至 100 岁,使用来自英格兰健康调查(2009-2012 年)和英国老龄化纵向研究(1998-2012 年)的数据,来模拟随着时间的推移模拟个体的风险因素变化。我们使用最近的项目数据来描述 NHS 健康检查的参与情况以及 4 种相关干预措施(他汀类药物、抗高血压药物、戒烟和体重管理)的参与情况。治疗效果和依从性的估计基于试验数据。我们估计了与没有系统健康检查的医疗保健系统相比,当前 NHS 健康检查计划的效益。这个反事实方案模拟了在“常规”初级保健中发生的风险因素的检测和治疗。我们还探讨了改变该计划的实施方式(包括资格、NHS 健康检查的参与情况和通过该计划提供的治疗方法的参与情况)的可行性。我们估计 NHS 健康检查计划可以预防 80 岁前 390 例(95%可信区间 290 至 500 例)过早死亡,并使每 100 万人中有 1370 人(95%可信区间 1100 至 1690 人)在 80 岁时免于疾病(缺血性心脏病、中风、痴呆和肺癌)。在队列的一生中(即,从 40-45 岁到 100 岁),这些变化导致额外增加 10000 个(95%可信区间 8200 至 13000)质量调整生命年(QALY)和额外增加 9000 年(6900 至 11300)的寿命。这相当于英格兰每年每 300 人减少约 30 例过早死亡和 1000 人免受这些疾病的影响。我们估计该计划目前每人头增加 3.8 天(95%可信区间 3.0-4.7)的 QALY,并在 60 年的随访期间增加 3.3 天(2.5-4.1)的存活时间。该计划对生活在最贫困地区的人群的健康影响比对生活在最贫困地区的人群的健康影响更大(每人头增加 4.4[2.7-6.5]天的额外质量调整生命与 2.8[1.7-4.0]天相比;每人头增加 5.1[3.4-7.1]天的额外寿命与 3.3[2.1-4.5]天相比)。改变现有计划的实施方式可能会导致效益显著增加。例如,一种策略是将高血压患者纳入计划,将可参与计划的年龄上限提高到 79 岁,将健康检查的参与率提高 30%,并将合格患者的治疗率提高 2.5 倍(即“最大潜力”方案),与当前计划相比,效益至少增加 3 倍(1360 例过早死亡与 390 例相比;5100 人免于 4 种疾病中的 1 种与 1370 例相比;37000 个额外的 QALY 与 10000 个相比;33000 个额外的寿命与 9000 个相比)。确保评估和有资格接受他汀类药物的患者接受他汀类药物是增加效益的一项重要策略。整体效益的估计基于当前的发病情况和管理情况,未来疾病发病率的下降或治疗效果的改善可能会改变长期观察到的实际效益。我们关注 NHS 健康检查计划的心血管部分。一些重要的非心血管健康结果(如戒烟预防慢性阻塞性肺疾病[COPD]和减肥预防癌症)和该计划的其他部分(如减少有害饮酒的简短干预措施)尚未建模。
我们的模型表明,目前的 NHS 健康检查计划正在改善健康状况并减少健康不平等。该计划的组织方式的改变可能会导致健康效益增加 3 倍以上。