Department of Global Health and Development, London School of Hygiene & Tropical Medicine, London, United Kingdom.
Sambodhi Research and Communications, Noida, Uttar Pradesh, India.
PLoS Med. 2018 Mar 6;15(3):e1002519. doi: 10.1371/journal.pmed.1002519. eCollection 2018 Mar.
To assess the effect of health information on immunisation uptake in rural India, we conducted an individually randomised controlled trial of health information messages targeting the mothers of unvaccinated or incompletely vaccinated children through home visits in rural Uttar Pradesh, India.
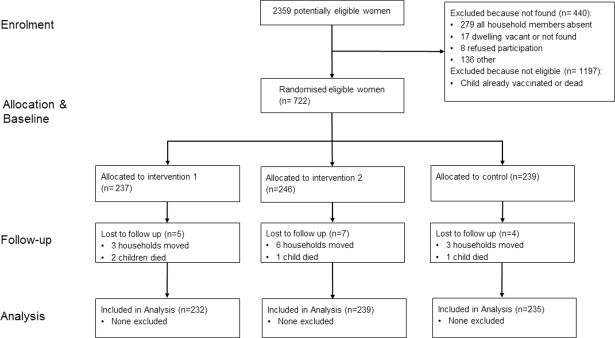
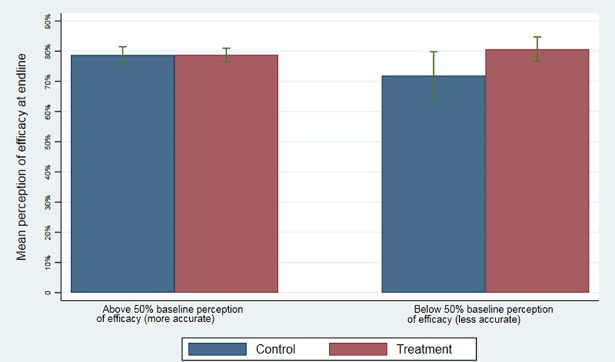
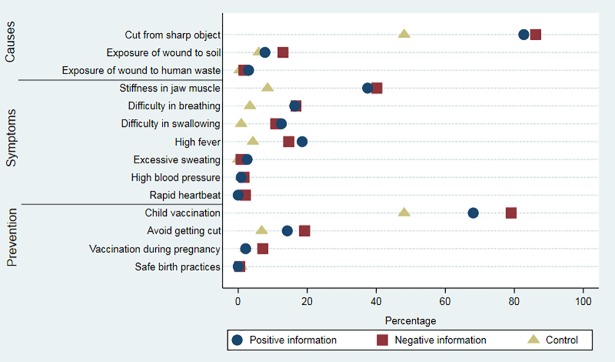
The study tested a brief intervention that provided mothers face-to-face with information on the benefits of the tetanus vaccine. Participants were 722 mothers of children aged 0-36 months who had not received 3 doses of diphtheria-pertussis-tetanus (DPT) vaccine (DPT3). Mothers were randomly assigned in a ratio of 1:1:1 to 1 of 3 study arms: mothers in the first treatment group received information framed as a gain (e.g., the child is less likely to get tetanus and more likely to be healthy if vaccinated), mothers in the second treatment group received information framed in terms of a loss (e.g., the child is more likely to get tetanus and suffer ill health if not vaccinated), and the third arm acted as a control group, with no information given to the mother. Surveys were conducted at baseline (September 2015) and after the intervention (April 2016). The primary outcome was the proportion of children who had received DPT3 measured after 7 months of follow-up. The analysis was by intention to treat. A total of 16 (2.2%) participants were lost to follow-up. The coverage of DPT3 was 28% in the control group and 43% in the pooled information groups, giving a risk difference of 15 percentage points (95% CI: 7% to 22%, p < 0.001) and a relative risk of 1.52 (95% CI: 1.2 to 1.9, p < 0.001). The information intervention increased the rate of measles vaccination by 22 percentage points (risk difference: 22%, 95% CI: 14% to 30%, p < 0.001; relative risk: 1.53, 95% CI: 1.29 to 1.80) and the rate of full immunisation by 14 percentage points (risk difference: 14%, 95% CI: 8% to 21%, p < 0.001; relative risk: 1.72, 95% CI: 1.29 to 2.29). It had a large positive effect on knowledge of the causes, symptoms, and prevention of tetanus but no effect on perceptions of vaccine efficacy. There was no difference in the proportion of children with DPT3 between the group that received information framed as a loss and the group that received information framed as a gain (risk difference: 4%, 95% CI: -5% to 13%; p = 0.352; relative risk: 1.11, 95% CI: 0.90 to 1.36). The cost per disability-adjusted life year averted of providing information was US$186, making the intervention highly cost-effective with respect to the WHO-recommended threshold of once the gross domestic product per capita (US$793 in the case of Uttar Pradesh). Key study limitations include the modest sample size for this trial, limiting power to detect small differences in the framing of information, and the potential for contamination among households.
Providing mothers of unvaccinated/incompletely vaccinated children with information on tetanus and the benefits of DPT vaccination substantially increased immunisation coverage and was highly cost-effective. The framing of the health information message did not appear to matter.
The trial is registered with ISRCTN, number ISRCTN84560580.
为了评估健康信息对印度农村地区免疫接种的影响,我们在印度北方邦农村地区进行了一项针对未接种或未完全接种疫苗的儿童的母亲的个体随机对照试验,通过家访向她们提供有关破伤风疫苗益处的健康信息。
该研究测试了一个简短的干预措施,通过面对面的方式向母亲提供有关破伤风疫苗益处的信息。研究对象为 722 名年龄在 0-36 个月之间、未接种 3 剂白喉-百日咳-破伤风(DPT)疫苗(DPT3)的儿童的母亲。母亲们按照 1:1:1 的比例随机分配到 3 个研究组之一:第一组治疗组接受的信息是基于收益的(例如,如果孩子接种了疫苗,患破伤风的可能性较小,更有可能健康),第二组治疗组接受的信息是基于损失的(例如,如果孩子未接种疫苗,患破伤风的可能性更大,健康状况更差),第三组作为对照组,母亲未收到任何信息。调查在基线(2015 年 9 月)和干预后(2016 年 4 月)进行。主要结局是在 7 个月的随访后接受 DPT3 的儿童比例。分析采用意向治疗。共有 16 名(2.2%)参与者失访。对照组的 DPT3 覆盖率为 28%,信息组的覆盖率为 43%,风险差异为 15 个百分点(95%CI:7%至 22%,p<0.001),相对风险为 1.52(95%CI:1.2 至 1.9,p<0.001)。信息干预措施使麻疹疫苗接种率提高了 22 个百分点(风险差异:22%,95%CI:14%至 30%,p<0.001;相对风险:1.53,95%CI:1.29 至 1.80),完全免疫接种率提高了 14 个百分点(风险差异:14%,95%CI:8%至 21%,p<0.001;相对风险:1.72,95%CI:1.29 至 2.29)。它对破伤风的病因、症状和预防的认识有很大的积极影响,但对疫苗效果的看法没有影响。在接受损失框架信息和接受收益框架信息的组之间,接受 DPT3 的儿童比例没有差异(风险差异:4%,95%CI:-5%至 13%;p=0.352;相对风险:1.11,95%CI:0.90 至 1.36)。提供信息以避免每一个残疾调整生命年的成本为 186 美元,相对于世界卫生组织建议的人均国内生产总值阈值(北方邦为 793 美元),该干预措施具有很高的成本效益。该试验的主要研究局限性包括试验样本量较小,限制了检测信息框架差异的能力,以及家庭之间存在潜在的污染。
为未接种/不完全接种疫苗的儿童的母亲提供有关破伤风和 DPT 疫苗接种益处的信息,大大提高了免疫接种覆盖率,且具有很高的成本效益。健康信息的呈现方式似乎并不重要。
该试验在 ISRCTN 注册,编号为 ISRCTN84560580。