Naiki Taku, Etani Toshiki, Naiki-Ito Aya, Fujii Kana, Ando Ryosuke, Iida Keitaro, Nagai Takashi, Sugiyama Yosuke, Nakagawa Motoo, Kawai Noriyasu, Yasui Takahiro
Department of Nephro-urology, Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan.
Department of Experimental Pathology and Tumor Biology, Nagoya City University Graduate School of Medical Sciences, Nagoya, Japan.
Case Rep Oncol. 2017 Nov 27;10(3):1057-1064. doi: 10.1159/000484597. eCollection 2017 Sep-Dec.
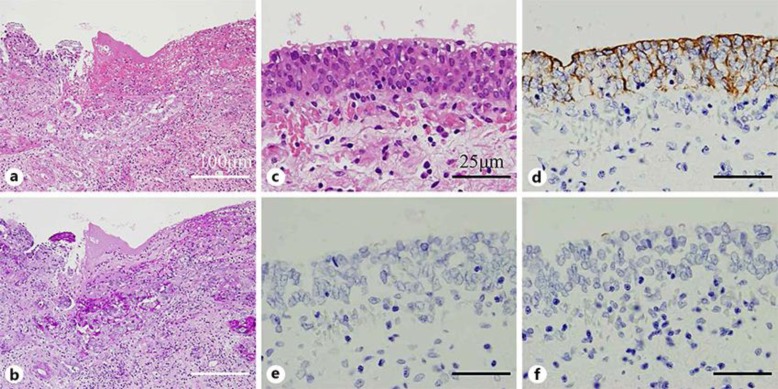
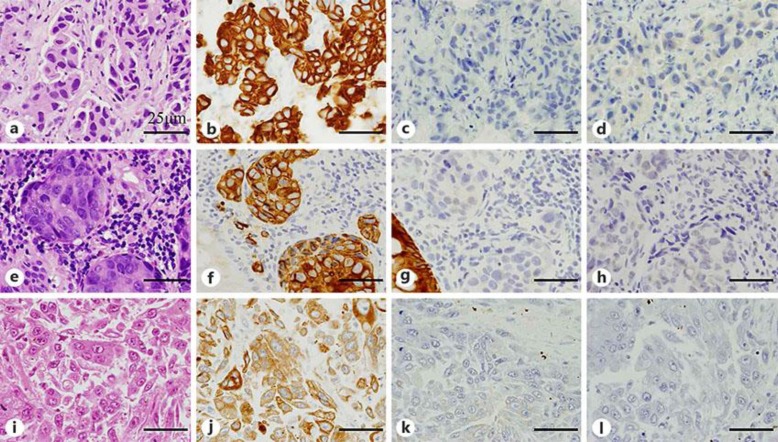
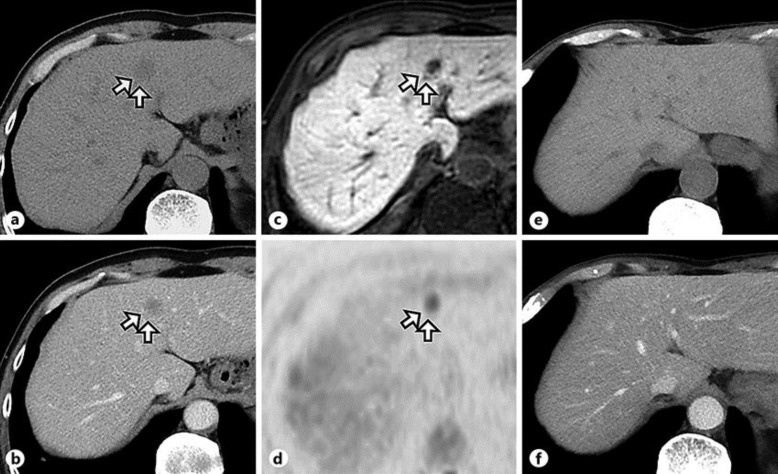
The prognostic significance of glandular differentiation in urothelial carcinoma (UC) is controversial, and thus far there is no established treatment strategy against metastasis of glandular component. We describe here a case of metastatic UC with glandular differentiation that had histological disappearance of adenocarcinoma components at autopsy after sequential chemotherapy with S-1 and cisplatin (CDDP) and with mFOLFOX6 (fluorouracil, oxaliplatin, and leucovorin) plus bevacizumab (mFOLFOX6+Bev). A 62-year-old Asian male was diagnosed with invasive UC with glandular differentiation (T2N0M0) by radical cystectomy and ileal conduit, and careful follow-up observation was made. Eight years after radical operation, peritoneal metastases occurred, and a biopsy specimen using colon fiber revealed high-grade adenocarcinomas with an immunohistochemical profile that included positivity for cytokeratin 7 (CK7) and negativity for cytokeratin 20 (CK20) and uroplakin, which was identical to the radical cystectomy specimen. Thus, he received combination chemotherapy consisting of S-1 and CDDP; however, the peritoneal metastasis worsened after 2 cycles. Therefore, second-line mFOLFOX6+Bev chemotherapy was performed for a total of 5 courses. In spite of this, the patient died, and the final diagnosis by autopsy was multiple metastases of infiltrating pure UC to the lung, bone, and peritoneum. Interestingly, there were no pathological findings of adenocarcinoma, and the immunohistochemical profile of the metastatic lesions was identical to that of the previous specimens from the bladder and colon. This suggests that sequential chemotherapy of S-1 and CDDP and second-line mFOLFOX6+Bev might be a feasible option in metastatic UC with glandular differentiation.
尿路上皮癌(UC)中腺性分化的预后意义存在争议,迄今为止,尚无针对腺性成分转移的确立治疗策略。我们在此描述一例具有腺性分化的转移性UC病例,该患者在先后接受S-1和顺铂(CDDP)以及mFOLFOX6(氟尿嘧啶、奥沙利铂和亚叶酸钙)联合贝伐单抗(mFOLFOX6+Bev)化疗后,尸检时腺癌成分出现组织学消失。一名62岁亚洲男性经根治性膀胱切除术和回肠导管术被诊断为具有腺性分化的浸润性UC(T2N0M0),并进行了仔细的随访观察。根治性手术后8年,出现腹膜转移,经结肠纤维活检标本显示为高级别腺癌,免疫组化特征包括细胞角蛋白7(CK7)阳性、细胞角蛋白20(CK20)和尿路上皮蛋白阴性,这与根治性膀胱切除标本相同。因此,他接受了S-1和CDDP的联合化疗;然而,2个周期后腹膜转移恶化。因此,进行了共5个疗程的二线mFOLFOX6+Bev化疗。尽管如此,患者仍死亡,尸检最终诊断为浸润性纯UC多发转移至肺、骨和腹膜。有趣的是,没有腺癌的病理表现,转移灶的免疫组化特征与先前膀胱和结肠标本的相同。这表明S-1和CDDP序贯化疗以及二线mFOLFOX6+Bev可能是具有腺性分化的转移性UC的一种可行选择。