Department of Emergency Medicine, University of British Columbia, Vancouver, British Columbia.
Centre for Clinical Epidemiology & Evaluation, Vancouver Coastal Health Research Institute, Vancouver, British Columbia.
Acad Emerg Med. 2018 Sep;25(9):1015-1026. doi: 10.1111/acem.13407.
Adverse drug events (ADEs) cause or contribute to one in nine emergency department (ED) presentations in North America and are often misdiagnosed. EDs have insufficient clinical pharmacists to complete medication reviews in all incoming patients, even though pharmacist-led medications reviews have been associated with improved health outcomes. Our objective was to validate clinical decision rules to identify patients presenting with ADEs so they could be prioritized for pharmacist-led medication review.
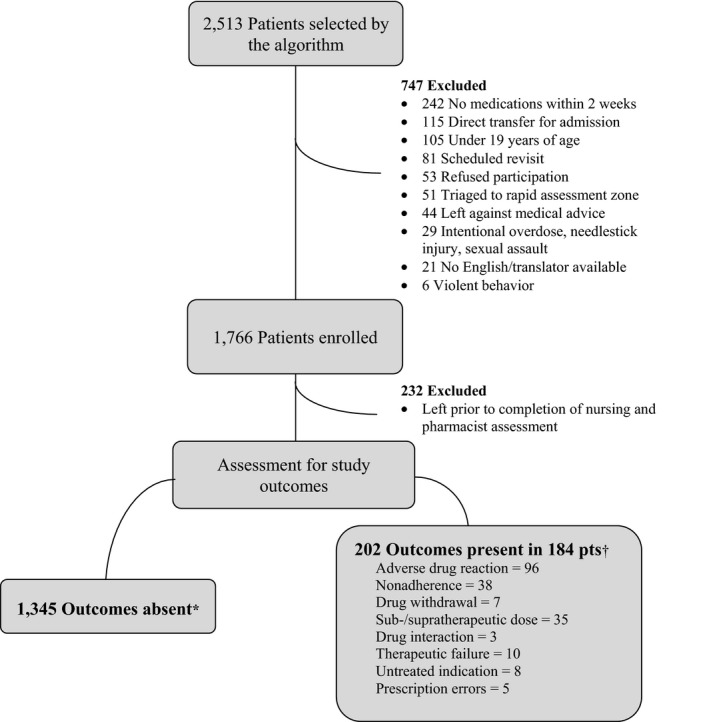
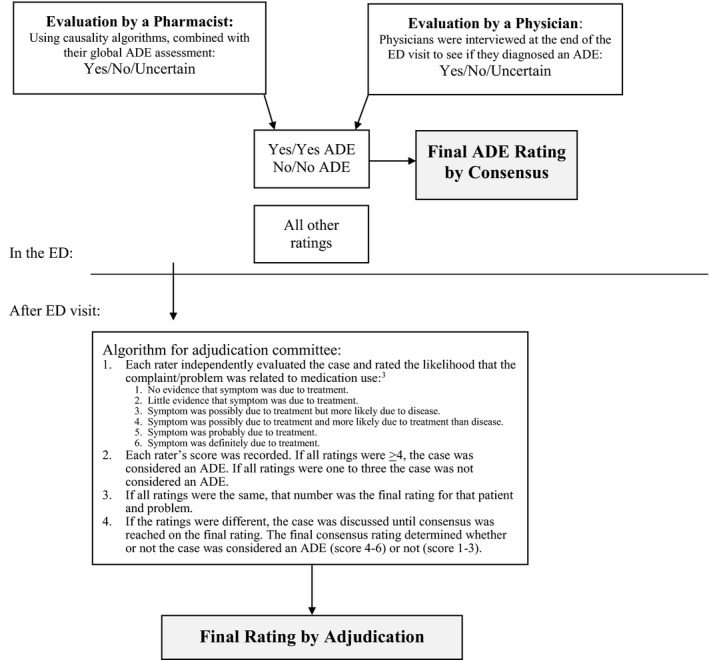
This multicenter, prospective study was conducted in two tertiary and one community hospital in Canada. We enrolled 1,529 adults presenting to EDs over 12 months. We applied two clinical decision rules and collected baseline variables prior to assessments by clinical pharmacists and physicians. We compared the physician and pharmacist diagnoses with the decision rule results. The primary outcome was a moderate or severe ADE, defined as an unintended and harmful event related to medication use or misuse, which required a change in medical therapy, diagnostic testing, consultation, or admission. An independent committee adjudicated uncertain and discordant cases. We calculated the diagnostic accuracy of both rules.
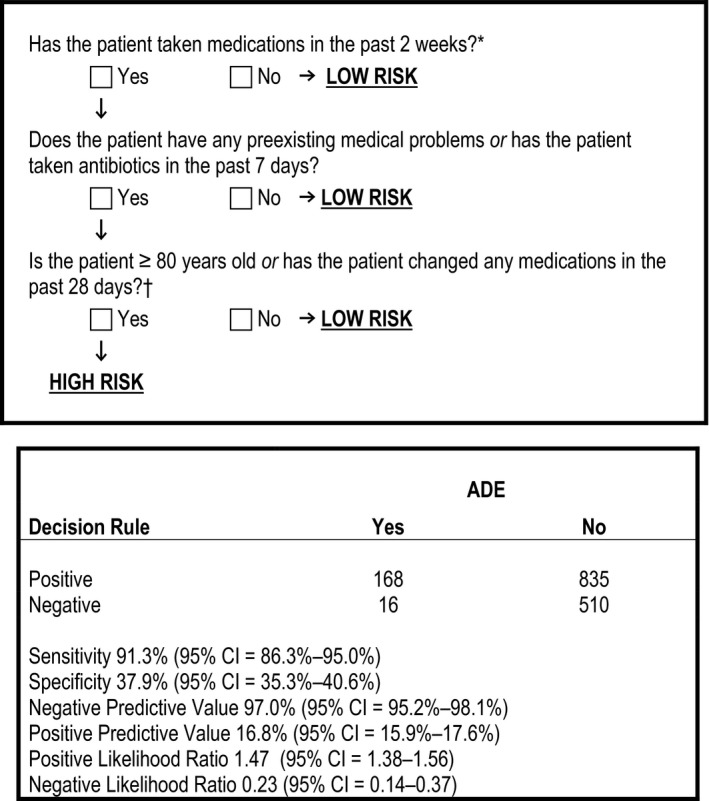
Among 1,529 patients, 184 (12.0%) were diagnosed with an ADE. Rule 1 contained the variables 1) having a preexisting medical condition or having taken antibiotics within 1 week and 2) age > 80 years or having a medication change within 28 days. They had a sensitivity of 91.3% (95% confidence interval [CI] = 86.3%-95.0%) and a specificity of 37.9% (95% CI = 35.3%-40.6%) for ADEs.
Our study validated clinical decision rules that can be applied by clinical pharmacists to limit the number of patients requiring medication review, while identifying the majority of patients presenting with clinically significant ADEs.
药物不良事件(ADE)导致或促成北美每九个急诊就诊(ED)中就有一个,并且经常被误诊。ED 缺乏足够的临床药师对所有来诊患者进行药物审查,尽管药师主导的药物审查与改善健康结果有关。我们的目标是验证临床决策规则,以确定出现 ADE 的患者,以便优先考虑由药师主导的药物审查。
这是一项在加拿大的两家三级医院和一家社区医院进行的多中心前瞻性研究。我们在 12 个月内招募了 1529 名成年 ED 就诊患者。我们应用了两种临床决策规则,并在临床药师和医生评估前收集了基线变量。我们将医生和药师的诊断与决策规则的结果进行了比较。主要结局是中度或重度 ADE,定义为与药物使用或误用相关的意外和有害事件,需要改变医疗治疗、诊断测试、咨询或入院。一个独立的委员会对不确定和不一致的病例进行了裁决。我们计算了这两种规则的诊断准确性。
在 1529 名患者中,有 184 名(12.0%)被诊断为 ADE。规则 1 包含以下变量:1)有预先存在的医疗状况或在 1 周内服用过抗生素;2)年龄>80 岁或在 28 天内有药物变化。它们对 ADE 的敏感性为 91.3%(95%置信区间[CI] = 86.3%-95.0%),特异性为 37.9%(95% CI = 35.3%-40.6%)。
我们的研究验证了临床决策规则,临床药师可以应用这些规则来限制需要药物审查的患者数量,同时识别出大多数出现有临床意义的 ADE 的患者。