Department of Radiation and Cellular Oncology, The University of Chicago Medicine, Chicago, Illinois, United States of America.
Department of Pathology, University of Utah/ARUP Laboratories, Salt Lake City, Utah, United States of America.
PLoS One. 2018 Mar 9;13(3):e0194234. doi: 10.1371/journal.pone.0194234. eCollection 2018.
Intensity-modulated radiation therapy (IMRT) has been used to limit treatment-related toxicity for patients with anal squamous cell carcinoma (SCC). The treatment outcomes and HPV characteristics for a cohort of patients receiving definitive concurrent chemotherapy and IMRT are reported.
52 patients with anal SCC were treated with IMRT and concurrent chemotherapy. Radiation was delivered sequentially to the pelvis and inguinal lymph nodes (45 Gy) and anal tumor (median dose, 54 Gy). Multiplex real-time PCR for 7 high-risk HPV subtypes (n = 22) and p16 immunohistochemistry (n = 21, rated on a 0, 1, and 2+ scale) were performed on available specimens. Survival was estimated using Kaplan-Meier analysis, and toxicities were recorded.
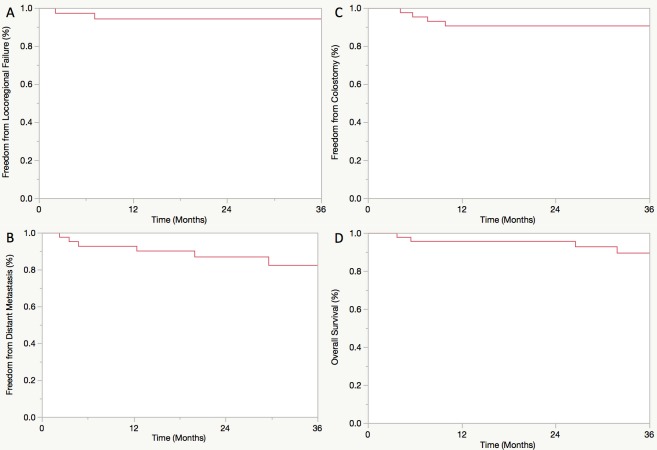
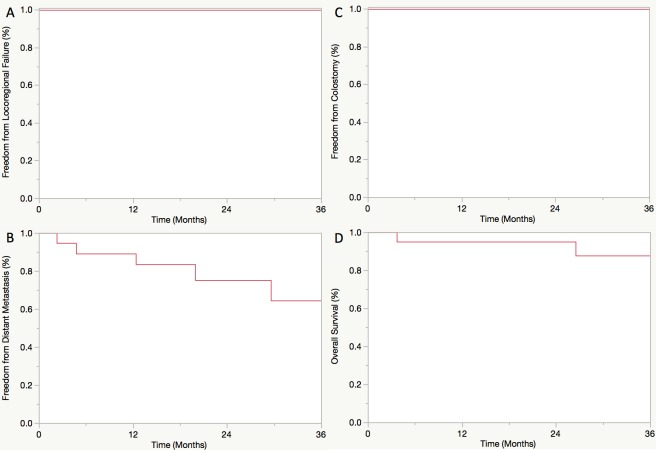
Median follow-up was 33 months. Three-year freedom from locoregional failure (FFLRF), freedom from distant metastasis (FFDM), freedom from colostomy (FFC), and overall survival (OS) were 94%, 85%, 91%, and 90%, respectively. Acute grade 2+ skin, GI, and GU toxicities occurred in 83%, 71%, and 19% of evaluable patients, respectively. The rates of late grade 2+ GI and GU toxicities for evaluable patients (n = 32) were 28% and 9%, respectively. Of patients with available pathology, 91% and 71% were positive for HPV and p16 (2+), respectively. HPV genotypes included 16 (n = 17), 33 (n = 2), 18 (n = 1), and 45 (n = 1). HPV and p16 status were associated on Chi-square analysis (p = 0.07). Neither HPV nor p16 status was significantly associated with any clinical outcome. For HPV+ patients, 3-year FFLRF, FFDM, FFC, and OS were 100%, 69%, 100%, and 88%, respectively.
In this patient cohort, disease control was excellent for anal SCC treated with definitive concurrent chemotherapy and IMRT, and treatment was well tolerated. HPV and p16 status were not prognostic for treatment outcomes which may be related to our small sample size.
调强放射治疗(IMRT)已被用于限制接受肛门鳞癌(SCC)治疗的患者的相关毒性。本文报告了一组接受根治性同步化疗和调强放疗的患者的治疗结果和 HPV 特征。
52 例肛门 SCC 患者接受 IMRT 和同步化疗。骨盆和腹股沟淋巴结(45Gy)和肛门肿瘤(中位剂量 54Gy)依次接受放射治疗。对可获得的标本进行 7 种高危 HPV 亚型(n=22)的多重实时 PCR 和 p16 免疫组化(n=21,评分 0、1 和 2+)。采用 Kaplan-Meier 分析法估计生存率,并记录毒性。
中位随访时间为 33 个月。3 年无局部区域失败(FFLRF)、无远处转移(FFDM)、无结肠造口术(FFC)和总生存率(OS)分别为 94%、85%、91%和 90%。可评估患者的急性 2+级皮肤、GI 和 GU 毒性发生率分别为 83%、71%和 19%。可评估患者(n=32)的晚期 2+级 GI 和 GU 毒性发生率分别为 28%和 9%。在有病理的患者中,HPV 和 p16(2+)阳性率分别为 91%和 71%。HPV 基因型包括 16(n=17)、33(n=2)、18(n=1)和 45(n=1)。HPV 和 p16 状态在卡方分析中具有相关性(p=0.07)。HPV 和 p16 状态与任何临床结果均无显著相关性。HPV+患者的 3 年 FFLRF、FFDM、FFC 和 OS 分别为 100%、69%、100%和 88%。
在本患者队列中,接受根治性同步化疗和调强放疗的肛门 SCC 患者的疾病控制效果非常好,且治疗耐受性良好。HPV 和 p16 状态与治疗结果无关,这可能与我们的小样本量有关。