Suzuki Kazuchika, Sakai Hiroaki, Takahashi Kenji
Department of Cardiovascular Surgery, Fujieda Municipal General Hospital, 4-1-11 Surugadai, Fujieda, Shizuoka, Japan.
Department of Anesthesia, Fujieda Municipal General Hospital, 4-1-11 Surugadai, Fujieda, Shizuoka, Japan.
JA Clin Rep. 2018;4(1):24. doi: 10.1186/s40981-018-0162-5. Epub 2018 Mar 5.
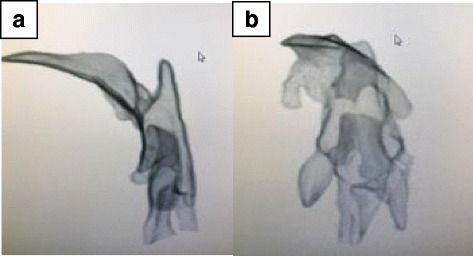
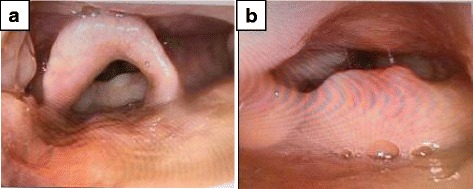
We herein report anesthetic management during aortic valve replacement for aortic valve regurgitation in a patient with adult mucopolysaccharidosis type II (MPS type 2) (Hunter syndrome). This disorder is rare and related to the accumulation of a mucopolysaccharide in lysosomes. It affects various organs, including the airways, heart, and central nerves. In children with MPS type 2, the risk of airway obstruction during anesthesia/sedation is high, and the degree of difficulty increases with aging. The patient described herein was a 33-year-old male without mental retardation. Before surgery, trismus, megaloglossia, and the disturbance of cervical vertebral excursion were noted, suggesting difficulties with ventilation/intubation. Anesthesia was induced under sedation/spontaneous respiration. A laryngeal deployment was conducted using a video laryngoscope; however, the Cormack grade was III. Nasotracheal fiber intubation was performed, and airway obstruction occurred. A muscle relaxant was administered, facilitating ventilation. However, subglottic stenosis, which was not detected before the surgery, made the tracheal tube insertion difficult. Aortic valve replacement was performed without complications. A detailed postoperative examination of the airways revealed oropharyngeal soft tissue outgrowth, narrowing of the upper airway, subglottic stenosis, and displacement/circumflex of the airway axis. Either awake intubation or rapid induction can be selected for this patient; however, either way have risks of airway obstruction. It is important that strategies under light anesthesia or incomplete neuromuscular blockade should be avoided for such our patient as suggested in the JSA airway management guidelines. A preoperative multidisciplinary airway assessment and simulation are important.
我们在此报告一例成年II型黏多糖贮积症(MPS 2型,亨特综合征)患者行主动脉瓣置换术治疗主动脉瓣反流时的麻醉管理。这种疾病较为罕见,与溶酶体中黏多糖的蓄积有关。它会影响包括气道、心脏和中枢神经在内的多个器官。在MPS 2型患儿中,麻醉/镇静期间气道梗阻的风险很高,且随着年龄增长难度增加。本文所述患者为一名33岁男性,无智力障碍。术前发现牙关紧闭、巨舌症和颈椎活动受限,提示通气/插管困难。在镇静/自主呼吸下诱导麻醉。使用可视喉镜进行喉暴露;然而,科马克分级为III级。进行了鼻气管纤维插管,出现气道梗阻。给予肌肉松弛剂以促进通气。然而,术前未检测到的声门下狭窄使气管导管插入困难。主动脉瓣置换术未出现并发症。术后对气道进行的详细检查发现口咽软组织增生、上气道狭窄、声门下狭窄以及气道轴线移位/弯曲。对于该患者,可以选择清醒插管或快速诱导;然而,两种方法都有气道梗阻的风险。正如日本麻醉学会气道管理指南所建议的,对于此类患者,应避免在浅麻醉或不完全神经肌肉阻滞下采取策略。术前多学科气道评估和模拟很重要。