Department of Hepatology, Graduate School of Medicine, Osaka City University, Osaka, Japan.
Department of Hepato-Biliary-Pancreatic Surgery, Graduate School of Medicine, Osaka City University, Osaka, Japan.
PLoS One. 2018 Mar 13;13(3):e0194163. doi: 10.1371/journal.pone.0194163. eCollection 2018.
Hepatocellular carcinoma (HCC) develops in some patients who achieve sustained virological response (SVR) against hepatitis C virus (HCV) infection via anti-HCV therapy. To examine the pathogenesis of HCC development after HCV eradication, histopathological changes and clinical markers were evaluated in SVR patients.
Of 654 SVR patients treated with interferon (IFN)-based therapies, 34 patients who had undergone liver biopsy before initiating IFN therapy and after SVR achievement were enrolled: 11 patients with HCC and 23 patients without HCC (male/female, 9/2 and 8/15, respectively: age, 58 ± 5 and 54 ± 11 years, respectively). We compared the clinical and histopathological factors between the two groups. Immunohistochemistry for Cytoglobin (CYGB) and α smooth muscle actin (α-SMA) was also performed.
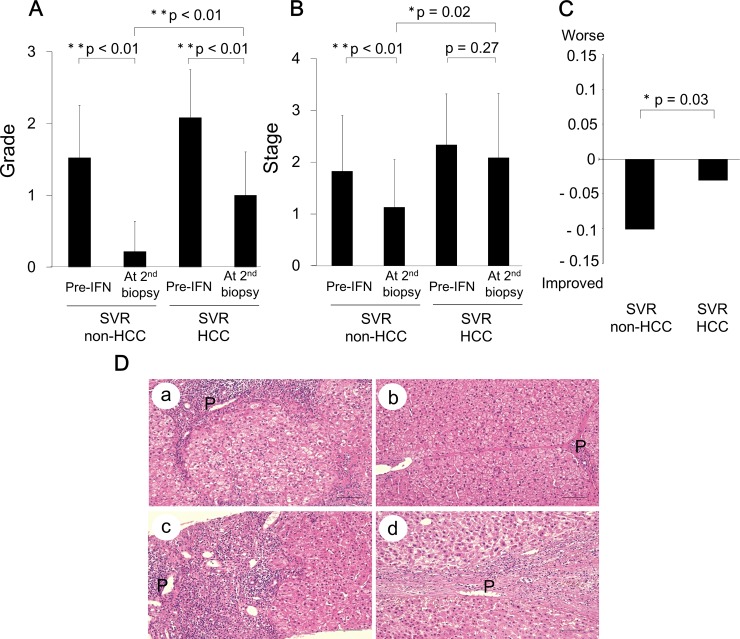
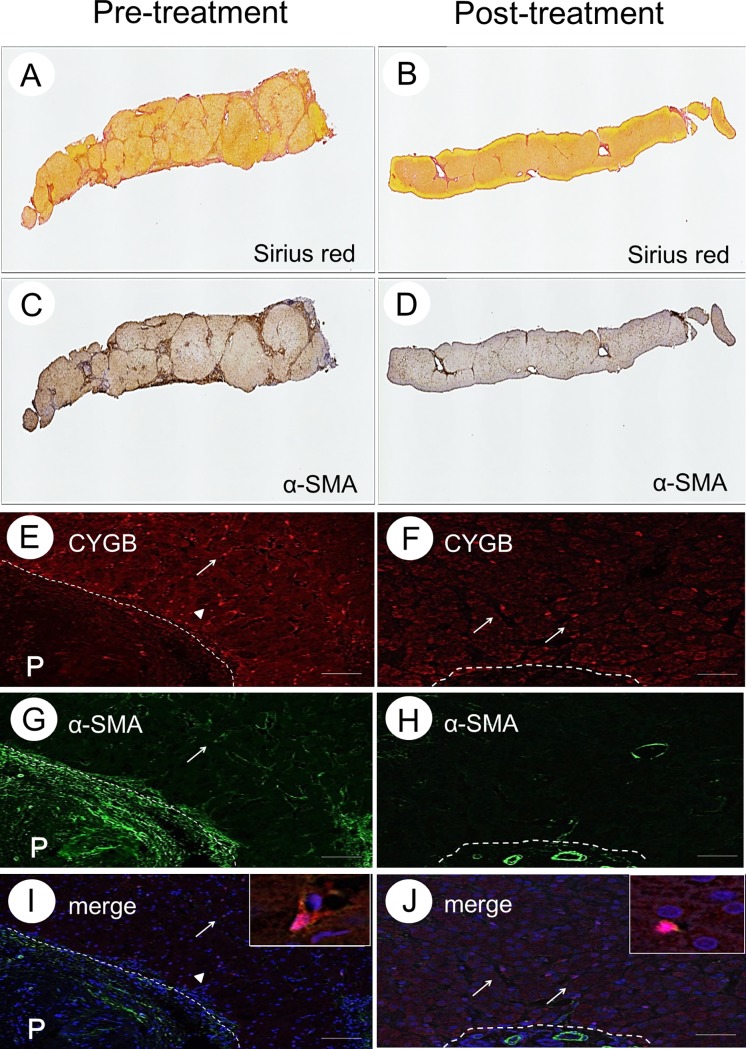
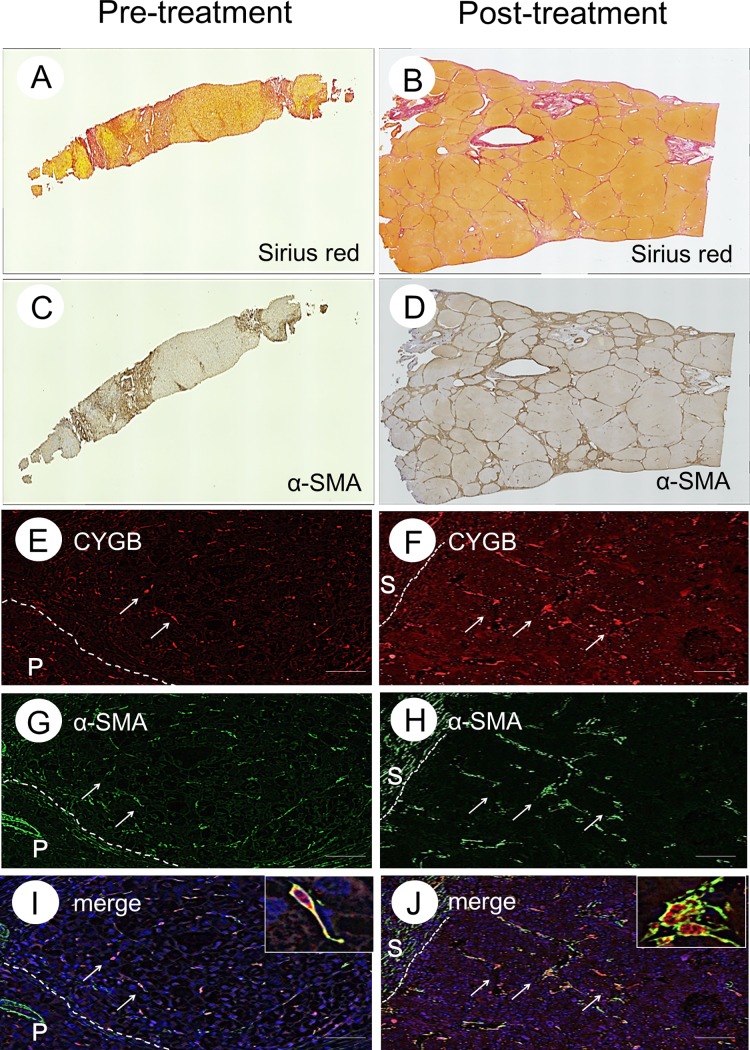
At baseline, prior to initiating the IFN-based therapy, there were significant differences between the SVR-non-HCC and SVR-HCC groups in the male gender, HBc antibody positivity, prothrombin activity, and histological inflammatory grade. Histopathological evaluation, using the new Inuyama classification system, revealed an improvement in the inflammatory grade, from 2.1 ± 0.6 to 1.0 ± 0.6 (p < 0.0001), whereas the fibrosis stage remained unchanged, from 2.3 ± 0.9 to 2.0 ± 1.2 (p = 0.2749), during the 97 ± 72-month observation period in the SVR-HCC group. Both the grade and stage scores were significantly improved in the SVR-non-HCC group. The area of collagen deposition, evaluated using Sirius red staining, showed a marked decrease, from 18.6 ± 7.6% to 7.7 ± 4.6%, in the SVR-non-HCC group, with no change in the SVR-HCC group. CYGB- and α-SMA-positive hepatic stellate cells (HSCs), indicative of the HSC activated phenotype, remained in the fibrotic tissue of livers among patients in the SVR-HCC group.
Stagnation of fibrosis regression is associated with a high risk for HCC after SVR. HSC activation may inhibit improvement in fibrosis after SVR and potentially contribute to hepatocarcinogenesis.
通过抗 HCV 治疗,一些慢性丙型肝炎病毒(HCV)感染患者实现持续病毒学应答(SVR)后,发展为肝细胞癌(HCC)。为了研究 HCV 清除后 HCC 发生的发病机制,对 SVR 患者进行了组织病理学变化和临床标志物的评估。
在接受干扰素(IFN)为基础的治疗的 654 例 SVR 患者中,纳入了 34 例在开始 IFN 治疗前和 SVR 获得后进行肝活检的患者:11 例 HCC 患者和 23 例非 HCC 患者(男/女,9/2 和 8/15,年龄,58 ± 5 和 54 ± 11 岁)。比较了两组的临床和组织病理学因素。还进行了细胞色素 b(CYGB)和α平滑肌肌动蛋白(α-SMA)的免疫组化染色。
在基线时,在开始 IFN 为基础的治疗之前,SVR-非 HCC 组和 SVR-HCC 组在男性、HBc 抗体阳性、凝血酶原活性和组织学炎症分级方面存在显著差异。使用新的 Inuyama 分类系统进行组织病理学评估显示,炎症分级从 2.1 ± 0.6 改善至 1.0 ± 0.6(p < 0.0001),而纤维化分期在 SVR-HCC 组的 97 ± 72 个月观察期内保持不变,从 2.3 ± 0.9 改善至 2.0 ± 1.2(p = 0.2749)。在 SVR-非 HCC 组中,胶原沉积面积(使用天狼猩红染色评估)从 18.6 ± 7.6%显著下降至 7.7 ± 4.6%,而 SVR-HCC 组无变化。CYGB 和 α-SMA 阳性的肝星状细胞(HSC),提示 HSC 激活表型,仍存在于 SVR-HCC 组患者的纤维化组织中。
纤维化消退停滞与 SVR 后 HCC 发生风险增加有关。HSC 激活可能会抑制 SVR 后纤维化的改善,并可能有助于肝癌的发生。