Internal Medicine Program, Jackson Memorial Hospital.
Division of Oncology, Department of Medicine, and.
Blood Adv. 2018 Mar 27;2(6):607-620. doi: 10.1182/bloodadvances.2017011106.
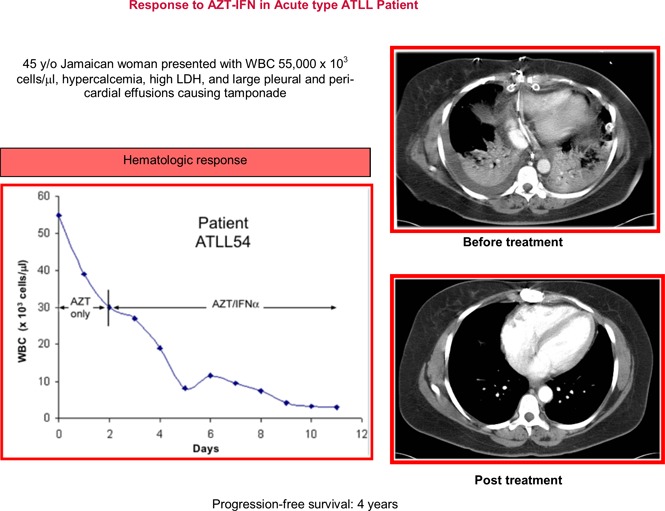
Adult T-cell leukemia/lymphoma (ATLL) is a fatal disease caused by human T-cell leukemia virus type 1 (HTLV-1). We retrospectively analyzed 195 patients with ATLL (lymphomatous n = 96, acute n = 80, unfavorable chronic n = 7, chronic n = 5, smoldering n = 3, and unclassified n = 4) diagnosed between 1987 and 2016 (median age 52 years, 77% Afro-Caribbean). Hypercalcemia was associated with acute ATLL (65%, vs 23% lymphomatous) ( = .012). The median survival for patients treated with modern therapies between 2000 and 2016 was 4.1 months for acute, 10.2 months for lymphomatous, 72 months for chronic/smoldering, and not reached for unfavorable chronic type, with 4-year survival rates of 10%, 4%, 60%, and 83%, respectively. The overall response rate (ORR) after first-line multiagent chemotherapy was 78% (complete response [CR] 39%) for acute vs 67% (CR 33%) for lymphomatous ATLL. First-line zidovudine interferon-α (AZT-IFN) resulted in ORR of 56% (CR 23%) for acute (n = 43), 33% (CR 16.5%) for lymphomatous (n = 6), and 86% (CR 29%) for unfavorable chronic ATLL. The median progression-free survival (PFS) in patients with aggressive ATLL who achieved CR after AZT-IFN was 48 months vs 11 months after chemotherapy ( = .003). Allogeneic hematopoietic stem cell transplant (allo-HSCT) resulted in a PFS of 24 and 28 months in 2 patients with lymphomatous ATLL. Our results suggest high-dose AZT-IFN is a reasonable up-front option for patients with aggressive leukemic ATLL followed by chemotherapy switch in nonresponders, whereas chemotherapy should be used in lymphomatous type followed by allo-HSCT when feasible.
成人 T 细胞白血病/淋巴瘤 (ATLL) 是一种致命疾病,由人类 T 细胞白血病病毒 1 型 (HTLV-1) 引起。我们回顾性分析了 195 例 ATLL 患者(淋巴母细胞型 n=96,急性型 n=80,预后不良慢性型 n=7,慢性型 n=5,冒烟型 n=3,未分类型 n=4),这些患者分别于 1987 年至 2016 年期间确诊(中位年龄 52 岁,77%为非裔加勒比人)。高钙血症与急性 ATLL 相关(65%,而淋巴母细胞型为 23%)(=.012)。2000 年至 2016 年期间接受现代治疗的患者的中位生存时间为急性型 4.1 个月,淋巴母细胞型 10.2 个月,慢性/冒烟型 72 个月,预后不良慢性型未达到,4 年生存率分别为 10%、4%、60%和 83%。一线多药化疗后的总体缓解率(ORR)为急性型 78%(完全缓解[CR]39%),淋巴母细胞型为 67%(CR 33%)。一线齐多夫定干扰素-α(AZT-IFN)治疗急性型的 ORR 为 56%(CR 23%)(n=43),淋巴母细胞型为 33%(CR 16.5%)(n=6),预后不良慢性型为 86%(CR 29%)。AZT-IFN 治疗后达到 CR 的急性侵袭性 ATLL 患者的中位无进展生存期(PFS)为 48 个月,而化疗后的中位 PFS 为 11 个月(=0.003)。2 例淋巴母细胞型 ATLL 患者接受异基因造血干细胞移植(allo-HSCT)后 PFS 分别为 24 个月和 28 个月。我们的研究结果表明,对于侵袭性白血病性 ATLL 患者,高剂量 AZT-IFN 是一种合理的一线治疗选择,对于无应答者,可在化疗后转换治疗;而对于淋巴母细胞型,在可行的情况下,应先进行化疗,然后进行 allo-HSCT。