Kattah Jorge C
Illinois Neurologic Institute, University of Illinois College of Medicine, Peoria, IL, United States.
Front Neurol. 2018 Mar 1;9:46. doi: 10.3389/fneur.2018.00046. eCollection 2018.
Previous series of bilateral vestibular loss (BVL) identified numerous etiologies, but surprisingly, a cause in a significant number of cases remains unknown. In an effort to understand possible etiology and management strategies, a global effort is currently in progress. Here, I contribute my 10-year experience with both acute and chronic BVL during the 2007-2017 decade.
This is a retrospective review of the charts and EMR of patients diagnosed with BVL in the last 10 years. Following Institutional IRB approval, we identified 57 patients with a diagnosis of BVL and utilized the current diagnostic criteria listed by the Barany society (1). The inclusion criteria included patients with BVL of any cause, within an age span older than 18 and a neuro-otologic examination supporting the clinical impression of BVL.
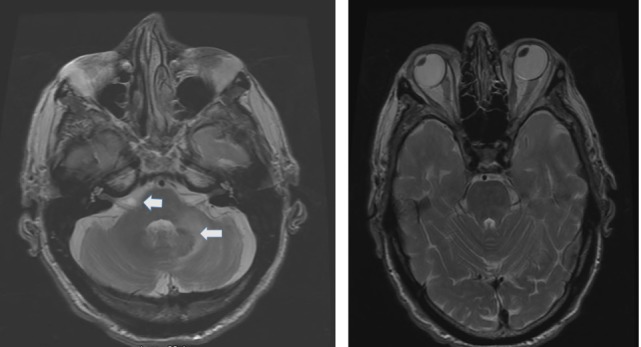
During the current decade 2007-2017, I identified two broad categories of BVL (acute and chronic) in 57 patients; only 41 of them had records available. The etiology includes: idiopathic: = 9, Wernicke's encephalopathy = 11, superficial siderosis = 3, paraneoplastic syndrome: = 3, bilateral vestibular neuritis (recurrent AVS lasting days without cochlear symptoms) = 3, simultaneous ototoxicity of aminoglycoside and chemotherapy toxicity = 2, MELAS = 2, Meniere's disease treated with intra-tympanic streptomycin in one ear = 1, acute phenytoin intoxication: = 1, combined chronic unilateral tumor-related vestibulopathy and new contralateral vestibular neuritis (this patient presented with Betcherew's phenomenon) = 1, bilateral AICA stroke = 1, mixed spinocerebellar ataxia type 3, = 2 and CANVAS = 2.
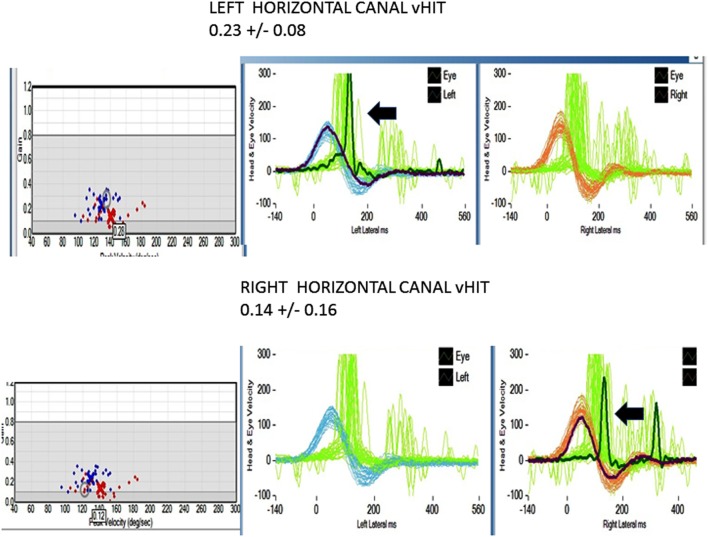
This cohort included a 28% overall incidence of acute and subacute BVL; among them, 65% improved with intervention. In the thiamine deficiency group, specifically, the vestibular function improved in 80% of the patients. Even though acute, subacute, or chronic showed slightly asymmetric horizontal-VOR gain loss, it never did cause spontaneous, primary straight gaze horizontal nystagmus. = 39/41 patients had abnormal manual HIT, = 26/41 BVL patients tested with video head impulse immediately after manual testing showed decreased VOR gain, including two with covert saccades. Two thiamine patients with positive bedside pretreatment manual HIT, tested after treatment with high-dose thiamine showed improved VOR. In acute thiamine deficiency, the horizontal VOR was abnormal and the vertical was either normal or mildly decreased. This series favored a neurologic cause of BVL. Finally, 20% of the chronic cases were idiopathic.
既往关于双侧前庭丧失(BVL)的系列研究确定了众多病因,但令人惊讶的是,相当一部分病例的病因仍不明。为了了解可能的病因及管理策略,目前正在全球范围内开展相关工作。在此,我分享一下2007年至2017年这十年间急性和慢性BVL的10年经验。
这是一项对过去10年诊断为BVL的患者病历和电子病历记录的回顾性研究。经机构审查委员会(IRB)批准后,我们确定了57例诊断为BVL的患者,并采用了巴拉尼协会列出的现行诊断标准(1)。纳入标准包括任何病因导致的BVL患者,年龄大于18岁,且神经耳科检查支持BVL的临床诊断。
在2007 - 2017这十年间,我在57例患者中确定了两大类BVL(急性和慢性);其中仅有41例有可用记录。病因包括:特发性 = 9例,韦尼克脑病 = 11例,浅表性铁沉积症 = 3例,副肿瘤综合征 = 3例,双侧前庭神经炎(复发性急性前庭综合征持续数天且无耳蜗症状) = 3例,氨基糖苷类药物和化疗毒性同时导致的耳毒性 = 2例,线粒体脑肌病伴乳酸血症和卒中样发作(MELAS) = 2例,一侧耳内注射链霉素治疗梅尼埃病 = 1例,急性苯妥英中毒 = 1例,慢性单侧肿瘤相关性前庭病变合并对侧新发性前庭神经炎(该患者出现贝切列夫现象) = 1例,双侧小脑前下动脉(AICA)卒中 = 1例,混合型脊髓小脑共济失调3型 = 2例,慢性非综合征性前庭病(CANVAS) = 2例。
该队列中急性和亚急性BVL的总体发病率为28%;其中,65%经干预后有所改善。具体而言在硫胺素缺乏组中,80%的患者前庭功能得到改善。尽管急性、亚急性或慢性病例均表现出水平半规管眼动反射(VOR)增益轻度不对称性丧失,但从未引起自发性、原发性直视水平性眼球震颤。41例患者中有39例手动头脉冲试验(HIT)异常,41例BVL患者在手动测试后立即进行视频头脉冲试验,其中26例显示VOR增益降低,包括2例伴有隐匿性扫视。2例床边硫胺素预处理手动HIT阳性的患者,在高剂量硫胺素治疗后进行测试,显示VOR有所改善。在急性硫胺素缺乏时,水平VOR异常,垂直VOR正常或轻度降低。该系列研究支持BVL的神经源性病因。最后,20%的慢性病例为特发性。