Al Moussawi Hassan, Krzyzak Michael, Awada Zainab, Chalhoub Jean M
Department of Medicine, Staten Island University Hospital, Northwell Health.
Cureus. 2018 Jan 13;10(1):e2061. doi: 10.7759/cureus.2061.
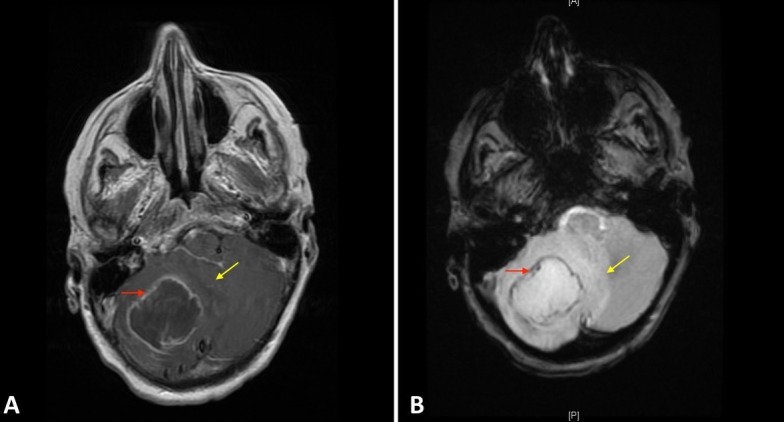
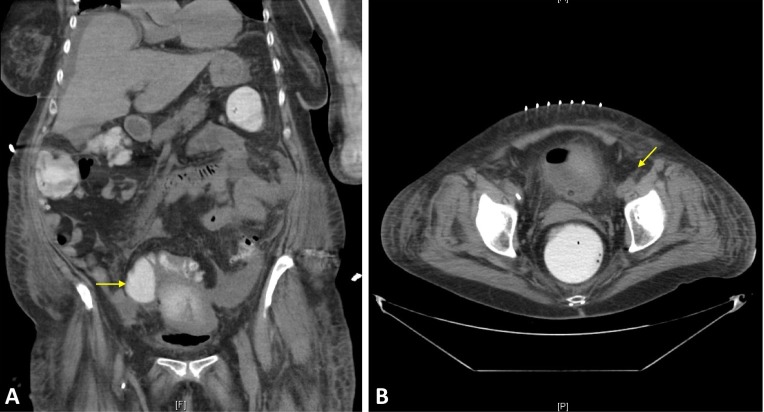
A brain abscess is defined as a focal intracerebral infection consisting of an encapsulated collection of pus, which can be a life-threatening complication of infections, trauma, or surgery. While immunocompromised patients can have a wide array of causative organisms, bacterial species represent the most common etiology in immunocompetent individuals. The incidence of brain abscesses ranges from 0.4 to 0.9 per 100,000, with a high predisposition among immunocompromised patients and in those with disruption of the blood-brain barrier. The most common causative organisms found were Streptococcus species, particularly S. viridians and S. pneumonia, Enterococcus, and Staphylococcus species, mainly S. aurieus and S. epidermidis. Microorganism can invade the brain through different mechanisms, either directly by contiguous spread and odontogenic infections, which usually cause a single brain abscess, or indirectly through hematogenous spread which can cause multiple brain abscesses. Both surgical and conservative dental procedures contribute to hematogenous spreading of oral microorganisms. Although most of those organisms are eliminated shortly after they gain access to the bloodstream, some can persist and contribute to the pathogenesis of abscesses in the appropriate environment. Odontogenic origins are rarely implicated in the formation of brain abscesses, and oral foci comprise approximately 5% of identified cases. We report a case of brain and diverticular abscesses due to S. intermidius occurring two months after dental extraction. This case highlights the fact that even usual dental workup can result in the development of bacteremia and disseminated abscesses including but not restricted to the brain. Consequently, in addition to identifying the possible source of bacteremia with an extensive history and physical exam, the diagnosis of Streptococcus milleri organisms should prompt the physicians to screen for sites of possible metastatic infection spread.
脑脓肿被定义为一种局灶性脑内感染,由包裹性脓液聚集构成,它可能是感染、创伤或手术的危及生命的并发症。虽然免疫功能低下的患者可能有多种致病微生物,但细菌种类是免疫功能正常个体中最常见的病因。脑脓肿的发病率为每10万人中有0.4至0.9例,在免疫功能低下的患者以及血脑屏障遭到破坏的患者中易感性较高。最常见的致病微生物是链球菌属,尤其是草绿色链球菌和肺炎链球菌、肠球菌以及葡萄球菌属,主要是金黄色葡萄球菌和表皮葡萄球菌。微生物可通过不同机制侵入大脑,要么直接通过邻近扩散和牙源性感染,这通常导致单个脑脓肿,要么间接通过血行播散,这可导致多个脑脓肿。外科和保守牙科手术都可导致口腔微生物的血行播散。虽然大多数这些微生物在进入血流后不久就会被清除,但有些可能会持续存在,并在适当环境中促成脓肿的发病机制。牙源性起源很少与脑脓肿的形成有关,口腔病灶约占已确诊病例的5%。我们报告一例拔牙后两个月因中间链球菌导致脑脓肿和憩室脓肿的病例。该病例突出了这样一个事实,即即使是常规牙科检查也可能导致菌血症和播散性脓肿的发生,包括但不限于脑部。因此除了通过详细的病史和体格检查确定可能的菌血症来源外,米勒链球菌属微生物的诊断应促使医生筛查可能发生转移性感染扩散的部位。