Cox Sharon E, Ellins Elizabeth A, Marealle Alphonce I, Newton Charles R, Soka Deogratias, Sasi Philip, Luca Di Tanna Gian, Johnson William, Makani Julie, Prentice Andrew M, Halcox Julian P, Kirkham Fenella J
Department of Population Health, London School of Hygiene & Tropical Medicine, London, UK; School of Tropical Medicine and Global Health, Nagasaki University, Nagasaki, Japan; Muhimbili Wellcome Programme, School of Medicine, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania.
Institute of Life Sciences, Swansea University Medical School, Swansea University, Swansea, UK.
Lancet Haematol. 2018 Apr;5(4):e147-e160. doi: 10.1016/S2352-3026(18)30020-6. Epub 2018 Mar 13.
Sickle-cell disease increases the risk of malnutrition. Low arginine and nitric oxide bioavailability are implicated in morbidity related to sickle-cell disease. Simple interventions are required, especially in low-income settings. We aimed to test the hypotheses that: (1) supplementary arginine, citrulline, and daily chloroquine increase bioavailable arginine and flow-mediated dilatation (FMD; maximal diameter change; FMD%), a measure of nitric oxide-dependent endothelial function; and (2) protein energy supplementation in the form of ready-to-use supplementary food (RUSF) improves the height-for-age and body-mass index-for-age Z-scores in children with sickle-cell disease.
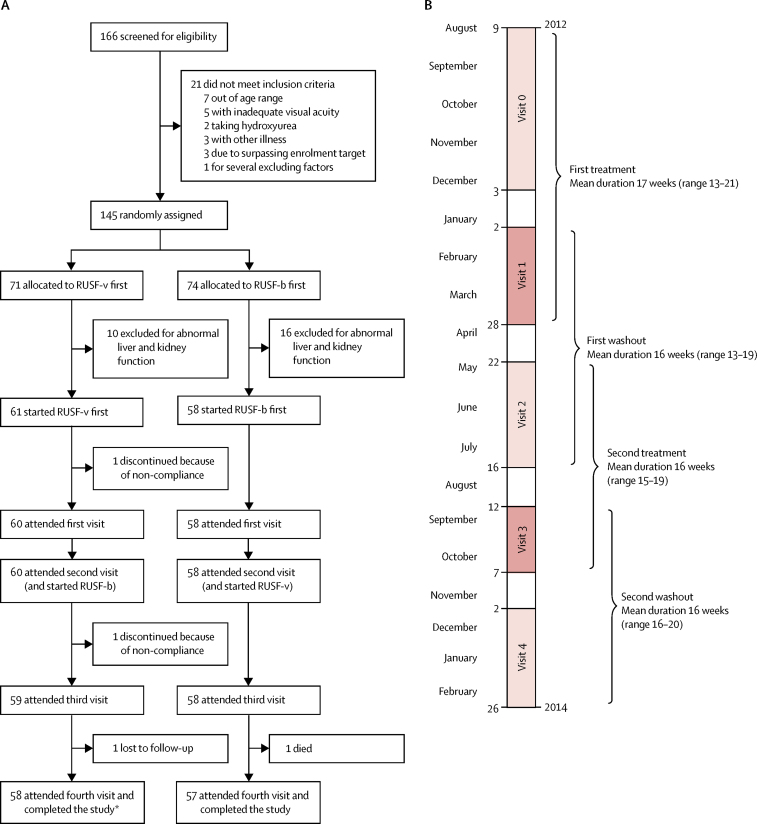
We performed a double-blind, random order crossover trial with two 4-month intervention periods (each followed by 4-month washout periods) in Muhimbili National Hospital in Dar-es-Salaam, Tanzania. We enrolled 119 children from the Muhimbili Sickle Cohort who were aged 8-12 years, naive to hydroxyurea, and had documented HbSS phenotype. Two formulations of RUSF (providing 500 kcal/day) were tested: basic (RUSF-b), with which children also received weekly chloroquine (150 mg or 225 mg chloroquine base, dependent on bodyweight); and vascular (RUSF-v), which was fortified with arginine and citrulline (designed to achieve mean intakes of 0·2 g/kg per day of arginine and 0·1 g/kg per day of citrulline), and with which children received daily chloroquine (maximum 3 mg chloroquine base/kg per day). Children were randomly allocated to receive either RUSF-b first or RUSF-v first and, after a washout period, were then given the other treatment. The primary outcomes in comparing the two RUSF formulations were mean plasma arginine, arginine to ornithine ratio, and arginine to asymmetric dimethylarginine ratio, and mean FMD%. The primary outcomes of the combined effect of both RUSF interventions were mean height-for-age Z-score and body-mass index-for-age Z-score. Analyses were done on the eligible intention-to-treat population. This trial is registered with ClinicalTrials.gov, number NCT01718054; and with ISRCTN74331412.
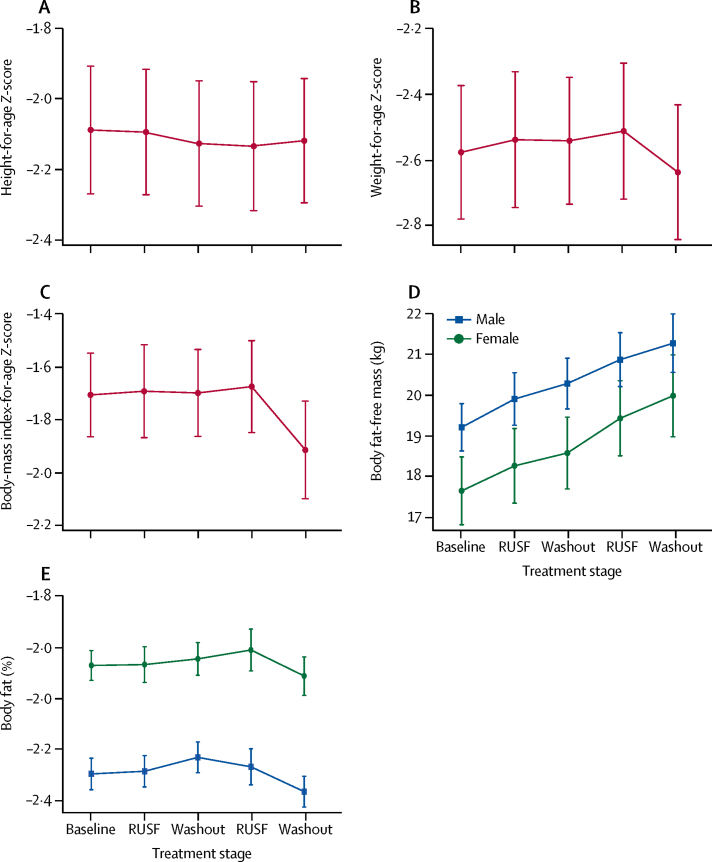
Between Aug 9, 2012, and Feb 26, 2014, 145 children were randomised (71 children to RUSF-v first and 74 children to RUSF-b first) and 119 children were treated, of whom 114 children yielded complete data for all reported endpoints. The ratio of arginine to ornithine (mean of individual differences -8·67%, 95% CI -19·55 to 2·20; p=0·12) and the mean FMD% (1·00, -0·47 to 2·47; p=0·18) did not significantly differ between the RUSF-b and RUSF-v treatments. However, the arginine to asymmetric dimethylarginine ratio was significantly increased by RUSF-v compared with RUSF-b (56·26%, 31·13 to 81·38; p<0·0001). In planned analyses that used mixed effects models to estimate the effect of each intervention compared with the participants at baseline or during washout periods, the arginine to asymmetric dimethylarginine ratio increased following both RUSF-v treatment (86%; p<0·0001) and RUSF-b treatment (40%; p<0·0001). However, FMD% was higher after treatment with RUSF-v (0·92; p<0·0001) but not RUSF-b (0·39; p=0·22). Following either intervention (RUSF-b and RUSF-v, pooled) body-mass index-for-age Z-score (0·091; p=0·001) and height-for-age Z-score (0·013; p=0·081) increased compared with baseline and washout timepoints. In 83 participants in the treated population, there were 71 adverse events during the intervention, of which 21 (30%) were serious, and 81 adverse events during the washout periods, of which 26 (32%) were serious (p=0·31), including one patient who died in the second washout period.
RUSF providing 500 kcal/day results in small weight gains in children with sickle-cell disease. However, even without arginine and citrulline fortification, RUSF seems to ameliorate arginine dysregulation and might improve endothelial function. Long-term studies are required to assess whether these physiological effects translate to improved clinical outcomes and better growth and development in patients with sickle-cell disease.
Wellcome Trust.
镰状细胞病会增加营养不良的风险。精氨酸和一氧化氮生物利用度低与镰状细胞病相关的发病率有关。需要采取简单的干预措施,尤其是在低收入环境中。我们旨在检验以下假设:(1)补充精氨酸、瓜氨酸和每日服用氯喹可提高生物可利用精氨酸水平以及血流介导的血管舒张功能(FMD;最大直径变化;FMD%),这是一种衡量一氧化氮依赖性内皮功能的指标;(2)以即用型补充食品(RUSF)形式进行的蛋白质能量补充可改善镰状细胞病患儿的年龄别身高和年龄别体重指数Z评分。
我们在坦桑尼亚达累斯萨拉姆的穆希姆比利国家医院进行了一项双盲、随机顺序交叉试验,设有两个为期4个月的干预期(每个干预期后均有4个月的洗脱期)。我们从穆希姆比利镰状细胞队列中招募了119名8至12岁、未使用过羟基脲且已记录为HbSS表型的儿童。测试了两种RUSF配方(每天提供500千卡能量):基本配方(RUSF-b),使用该配方的儿童还每周服用氯喹(150毫克或225毫克氯喹碱,取决于体重);血管配方(RUSF-v),该配方添加了精氨酸和瓜氨酸(旨在实现每天每千克体重平均摄入0.2克精氨酸和0.1克瓜氨酸),使用该配方的儿童每天服用氯喹(最大剂量为每天每千克体重3毫克氯喹碱)。儿童被随机分配先接受RUSF-b或先接受RUSF-v,经过洗脱期后,再接受另一种治疗。比较两种RUSF配方的主要结局指标为平均血浆精氨酸、精氨酸与鸟氨酸的比值、精氨酸与不对称二甲基精氨酸的比值以及平均FMD%。两种RUSF干预措施联合效果的主要结局指标为平均年龄别身高Z评分和年龄别体重指数Z评分。分析是在符合条件的意向性治疗人群中进行的。该试验已在ClinicalTrials.gov注册,注册号为NCT01718054;并在ISRCTN注册,注册号为74331412。
在2012年8月9日至2014年2月26日期间,145名儿童被随机分组(71名儿童先接受RUSF-v,74名儿童先接受RUSF-b),119名儿童接受了治疗,其中114名儿童提供了所有报告终点的完整数据。RUSF-b和RUSF-v治疗之间,精氨酸与鸟氨酸的比值(个体差异均值为 -8.67%,95%置信区间为 -19.55至2.20;p = 0.12)和平均FMD%(1.00,-0.47至2.47;p = 0.18)无显著差异。然而,与RUSF-b相比,RUSF-v使精氨酸与不对称二甲基精氨酸的比值显著升高(升高56.26%,95%置信区间为31.13至81.38;p < 0.0001)。在使用混合效应模型估计每种干预措施与基线或洗脱期参与者相比的效果的计划分析中,RUSF-v治疗后(升高86%;p < 0.0001)和RUSF-b治疗后(升高40%;p < 0.0001)精氨酸与不对称二甲基精氨酸的比值均升高。然而,RUSF-v治疗后FMD%较高(0.92;p < 0.0001),而RUSF-b治疗后则不然(0.39;p = 0.22)。与基线和洗脱期时间点相比,无论采用哪种干预措施(RUSF-b和RUSF-v合并),年龄别体重指数Z评分(升高0.091;p = 0.001)和年龄别身高Z评分(升高0.013;p = 0.081)均有所升高。在接受治疗的人群中,83名参与者在干预期间发生了71起不良事件,其中21起(30%)为严重不良事件,在洗脱期发生了81起不良事件,其中26起(32%)为严重不良事件(p = 0.31),包括1名患者在第二个洗脱期死亡。
每天提供500千卡能量的RUSF可使镰状细胞病患儿体重略有增加。然而,即使未添加精氨酸和瓜氨酸,RUSF似乎也能改善精氨酸失调,并可能改善内皮功能。需要进行长期研究,以评估这些生理效应是否能转化为镰状细胞病患者更好的临床结局以及更好的生长发育。
惠康信托基金会。