Gripp Eliza de Almeida, Oliveira Gabriela Escudini de, Feijó Luiz Augusto, Garcia Marcelo Iorio, Xavier Sergio Salles, Sousa Andréa Silvestre de
Hospital Universitário Clementino Fraga Filho - Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ - Brazil.
Arq Bras Cardiol. 2018 Feb;110(2):140-150. doi: 10.5935/abc.20180021.
The high cardiotoxicity morbidity and mortality rates associated with the antineoplastic therapy for breast cancer could be reduced with the early use of cardioprotective drugs. However, the low sensitivity of left ventricular ejection fraction limits its use in that preventive strategy. New parameters, such as global longitudinal strain, are being used in the early detection of contractile function changes.
To assess the incidence of cardiotoxicity in patients treated for breast cancer, the independent factors associated with that event, and the ability of strain to identify it early.
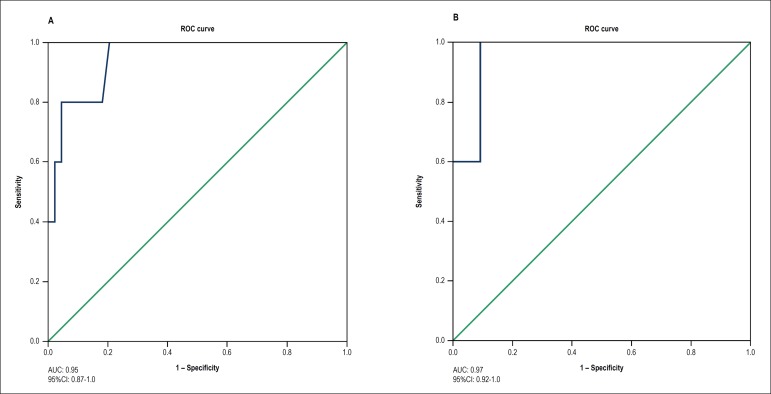
Prospective observational study of consecutive outpatients diagnosed with breast cancer, with no previous antineoplastic treatment and no ventricular dysfunction, who underwent anthracycline and/or trastuzumab therapy. The patients were quarterly evaluated on a 6- to 12-month follow-up by an observer blind to therapy. Cox regression was used to evaluate the association of cardiotoxicity with clinical, therapeutic and echocardiographic variables. A ROC curve was built to identify the strain cutoff point on the third month that could predict the ejection fraction reduction on the sixth month. For all tests, the statistical significance level adopted was p ≤ 0.05.
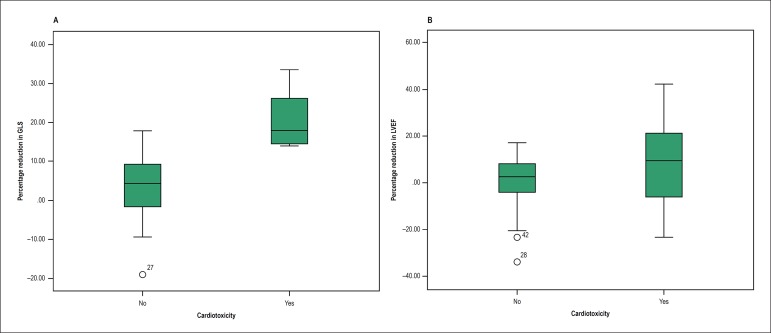
Of 49 women (mean age, 49.7 ± 12.2 years), cardiotoxicity was identified in 5 (10%) on the third (n = 2) and sixth (n = 3) months of follow-up. Strain was independently associated with the event (p = 0.004; HR = 2.77; 95%CI: 1.39-5.54), with a cutoff point for absolute value of -16.6 (AUC = 0.95; 95%CI: 0.87-1.0) or a cutoff point for percentage reduction of 14% (AUC = 0.97; 95%CI: 0.9-1.0).
The 14% reduction in strain (absolute value of -16.6) allowed the early identification of patients who could develop anthracycline and/or trastuzumab-induced cardiotoxicity.
早期使用心脏保护药物可降低与乳腺癌抗肿瘤治疗相关的高心脏毒性发病率和死亡率。然而,左心室射血分数的低敏感性限制了其在该预防策略中的应用。诸如整体纵向应变等新参数正被用于收缩功能变化的早期检测。
评估接受乳腺癌治疗的患者中心脏毒性的发生率、与该事件相关的独立因素以及应变早期识别心脏毒性的能力。
对连续的门诊乳腺癌患者进行前瞻性观察研究,这些患者既往未接受过抗肿瘤治疗且无心室功能障碍,接受了蒽环类药物和/或曲妥珠单抗治疗。由对治疗不知情的观察者在6至12个月的随访中每季度对患者进行评估。采用Cox回归评估心脏毒性与临床、治疗及超声心动图变量之间的关联。构建ROC曲线以确定第三个月时可预测第六个月射血分数降低的应变截断点。对于所有检验,采用的统计学显著性水平为p≤0.05。
49名女性(平均年龄49.7±12.2岁)中,在随访的第三个月(n = 2)和第六个月(n = 3)发现5例(10%)出现心脏毒性。应变与该事件独立相关(p = 0.004;HR = 2.77;95%CI:1.39 - 5.54),绝对值的截断点为 - 16.6(AUC = 0.95;95%CI:0.87 - 1.0)或百分比降低的截断点为14%(AUC = 0.97;95%CI:0.9 - 1.0)。
应变降低14%(绝对值为 - 16.6)可早期识别可能发生蒽环类药物和/或曲妥珠单抗诱导的心脏毒性的患者。