Varricchi Gilda, Ameri Pietro, Cadeddu Christian, Ghigo Alessandra, Madonna Rosalinda, Marone Giancarlo, Mercurio Valentina, Monte Ines, Novo Giuseppina, Parrella Paolo, Pirozzi Flora, Pecoraro Antonio, Spallarossa Paolo, Zito Concetta, Mercuro Giuseppe, Pagliaro Pasquale, Tocchetti Carlo G
Department of Translational Medical Sciences, University of Naples Federico II, Naples, Italy.
Department of Translational Medical Sciences, Center for Basic and Clinical Immunology Research, University of Naples Federico II, Naples, Italy.
Front Physiol. 2018 Mar 7;9:167. doi: 10.3389/fphys.2018.00167. eCollection 2018.
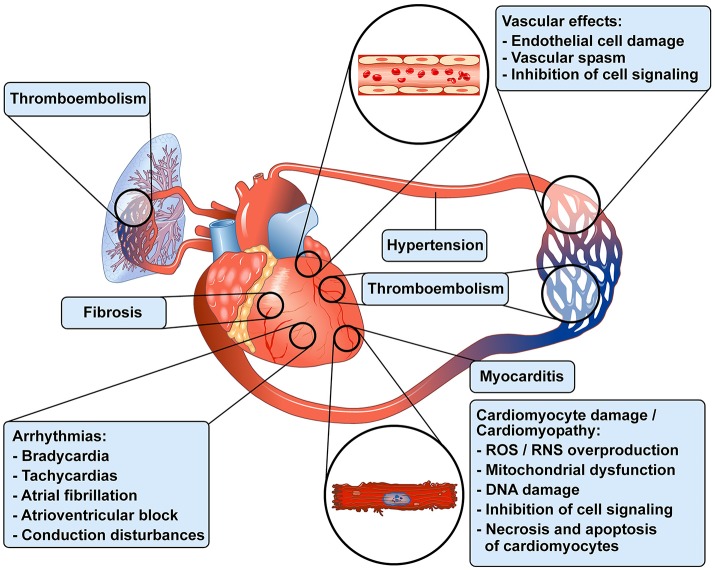
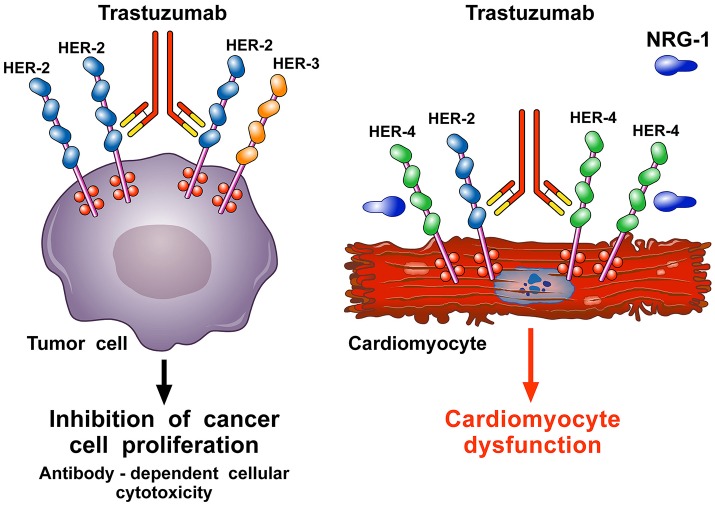
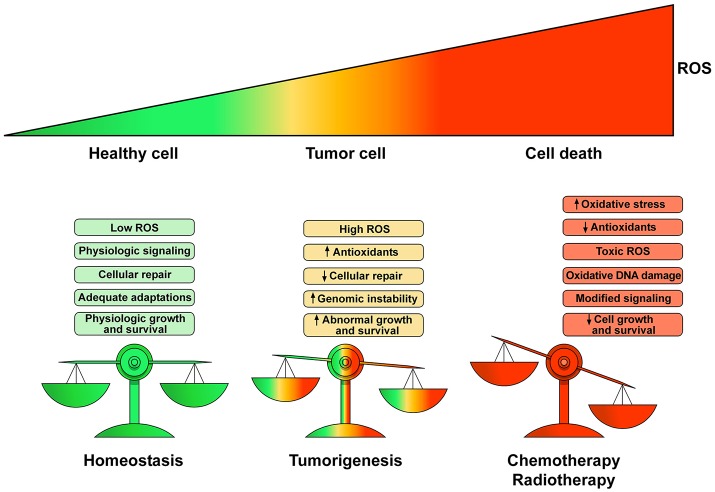
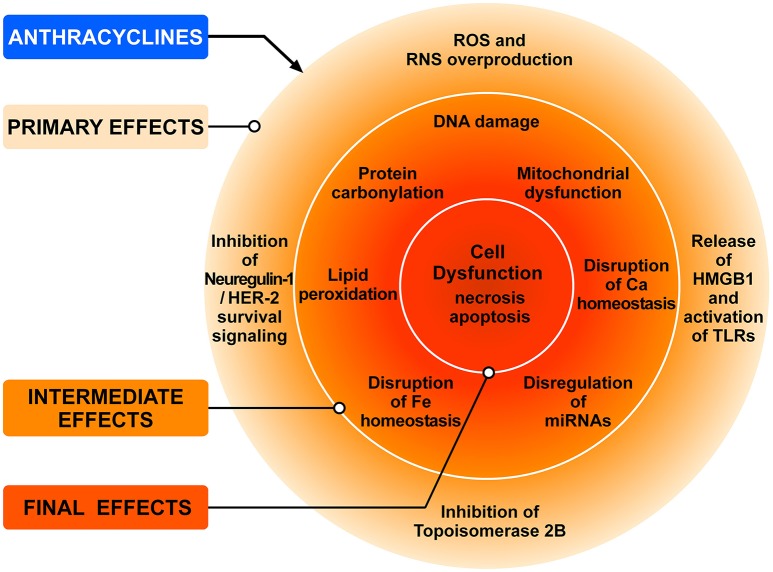
Antineoplastic drugs can be associated with several side effects, including cardiovascular toxicity (CTX). Biochemical studies have identified multiple mechanisms of CTX. Chemoterapeutic agents can alter redox homeostasis by increasing the production of reactive oxygen species (ROS) and reactive nitrogen species RNS. Cellular sources of ROS/RNS are cardiomyocytes, endothelial cells, stromal and inflammatory cells in the heart. Mitochondria, peroxisomes and other subcellular components are central hubs that control redox homeostasis. Mitochondria are central targets for antineoplastic drug-induced CTX. Understanding the mechanisms of CTX is fundamental for effective cardioprotection, without compromising the efficacy of anticancer treatments. Type 1 CTX is associated with irreversible cardiac cell injury and is typically caused by anthracyclines and conventional chemotherapeutic agents. Type 2 CTX, associated with reversible myocardial dysfunction, is generally caused by biologicals and targeted drugs. Although oxidative/nitrosative reactions play a central role in CTX caused by different antineoplastic drugs, additional mechanisms involving directly and indirectly cardiomyocytes and inflammatory cells play a role in cardiovascular toxicities. Identification of cardiologic risk factors and an integrated approach using molecular, imaging, and clinical data may allow the selection of patients at risk of developing chemotherapy-related CTX. Although the last decade has witnessed intense research related to the molecular and biochemical mechanisms of CTX of antineoplastic drugs, experimental and clinical studies are urgently needed to balance safety and efficacy of novel cancer therapies.
抗肿瘤药物可能会引发多种副作用,包括心血管毒性(CTX)。生化研究已确定了CTX的多种机制。化疗药物可通过增加活性氧(ROS)和活性氮(RNS)的生成来改变氧化还原稳态。ROS/RNS的细胞来源包括心肌细胞、内皮细胞、心脏中的基质细胞和炎性细胞。线粒体、过氧化物酶体和其他亚细胞成分是控制氧化还原稳态的核心枢纽。线粒体是抗肿瘤药物诱导的CTX的主要靶点。了解CTX的机制对于有效的心脏保护至关重要,同时又不影响抗癌治疗的疗效。1型CTX与不可逆的心脏细胞损伤相关,通常由蒽环类药物和传统化疗药物引起。2型CTX与可逆性心肌功能障碍相关,一般由生物制剂和靶向药物引起。尽管氧化/亚硝化反应在不同抗肿瘤药物引起的CTX中起核心作用,但涉及直接和间接心肌细胞及炎性细胞的其他机制也在心血管毒性中发挥作用。识别心脏危险因素并采用分子、影像学和临床数据的综合方法,可能有助于选择有发生化疗相关CTX风险的患者。尽管在过去十年中,针对抗肿瘤药物CTX的分子和生化机制进行了深入研究,但仍迫切需要进行实验和临床研究,以平衡新型癌症治疗的安全性和有效性。