Han Jun, Won Seok-Hyung, Kim Jung-Taek, Hahn Myung-Hoon, Won Ye-Yeon
Department of Orthopaedic Surgery, Ajou University College of Medicine, Suwon, Korea.
Department of Orthopaedic, Cheil General Hospital and Women's Healthcare Center, Dankook University College of Medicine, Cheonan, Korea.
Hip Pelvis. 2018 Mar;30(1):5-11. doi: 10.5371/hp.2018.30.1.5. Epub 2018 Mar 5.
Femoroacetabular impingement (FAI) is considered an important cause of early degenerative arthritis development. Although three-dimensional (3D) imaging such as computed tomography (CT) and magnetic resonance imaging are considered precise imaging modalities for 3D morphology of FAI, they are associated with several limitations when used in out-patient clinics. The paucity of FAI morphologic data in Koreans makes it difficult to select the most effective radiographical method when screening for general orthopedic problems. We postulate that there might be an individual variation in the distribution of cam deformity in the asymptomatic Korean population.
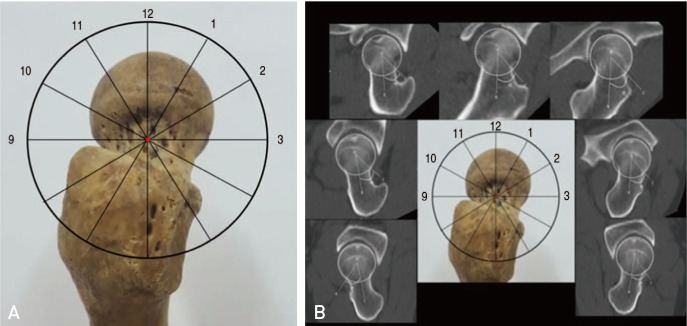
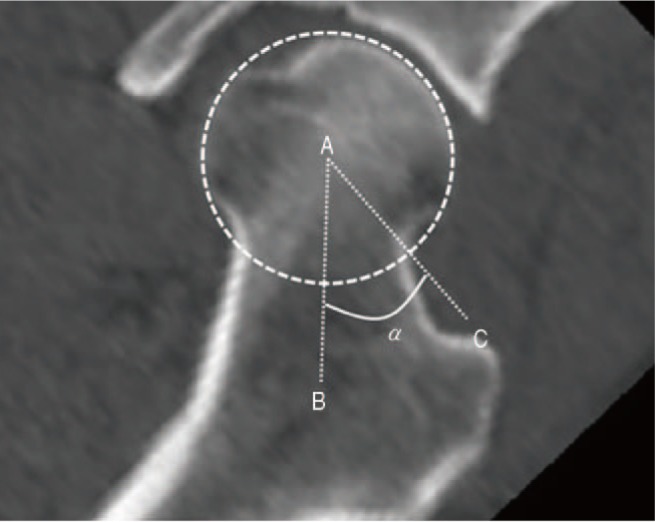
From January 2011 to December 2015, CT images of the hips of 100 subjects without any history of hip joint ailments were evaluated. A computer program which generates 3D models from CT scans was used to provide sectional images which cross the central axis of the femoral head and neck. Alpha angles were measured in each sectional images. Alpha angles above 55° were regarded as cam deformity.
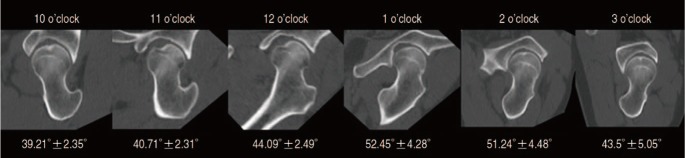
The mean alpha angle was 43.5°, range 34.7-56.1°(3 o'clock); 51.24°, range 39.5-58.8°(2 o'clock); 52.45°, range 43.3-65.5°(1 o'clock); 44.09°, range 36.8-49.8°(12 o'clock); 40.71, range 33.5-45.8°(11 o'clock); and 39.21°, range 34.1-44.6°(10 o'clock). Alpha angle in 1 and 2 o'clock was significantly larger than other locations (<0.01). The prevalence of cam deformity was 18.0% and 19.0% in 1 and 2 o'clock, respectively.
Cam deformity of FAI was observed in 31% of asymptomatic hips. The most common region of cam deformity was antero-superior area of femoral head-neck junction (1 and 2 o'clock).
股骨髋臼撞击症(FAI)被认为是早期退行性关节炎发展的重要原因。尽管诸如计算机断层扫描(CT)和磁共振成像等三维(3D)成像被视为用于FAI三维形态的精确成像方式,但在门诊使用时它们存在一些局限性。韩国人FAI形态学数据的匮乏使得在筛查一般骨科问题时难以选择最有效的影像学方法。我们推测无症状韩国人群中凸轮畸形的分布可能存在个体差异。
对2011年1月至2015年12月期间100名无任何髋关节疾病史的受试者的髋关节CT图像进行评估。使用一个从CT扫描生成3D模型的计算机程序来提供穿过股骨头和颈中轴线的断层图像。在每个断层图像上测量阿尔法角。阿尔法角大于55°被视为凸轮畸形。
平均阿尔法角在3点位置为43.5°,范围34.7 - 56.1°;2点位置为51.24°,范围39.5 - 58.8°;1点位置为52.45°,范围43.3 - 65.5°;12点位置为44.09°,范围36.8 - 49.8°;11点位置为40.71°,范围33.5 - 45.8°;10点位置为39.21°,范围34.1 - 44.6°。1点和2点位置的阿尔法角显著大于其他位置(<0.01)。1点和2点位置凸轮畸形的患病率分别为18.0%和19.0%。
在31%的无症状髋关节中观察到FAI的凸轮畸形。凸轮畸形最常见的区域是股骨头 - 颈交界处的前上方区域(1点和2点位置)。