Kampondeni Samuel D, Birbeck Gretchen L, Seydel Karl B, Beare Nicholas A, Glover Simon J, Hammond Colleen A, Chilingulo Cowles A, Taylor Terrie E, Potchen Michael J
Blantyre Malaria Project, University of Malawi College of Medicine, Chichiri, Blantyre, Malawi.
Department of Imaging Sciences, Division of Diagnostic and Interventional Neuroradiology, University of Rochester Medical Center, Rochester, New York.
Surg Neurol Int. 2018 Mar 1;9:53. doi: 10.4103/sni.sni_297_17. eCollection 2018.
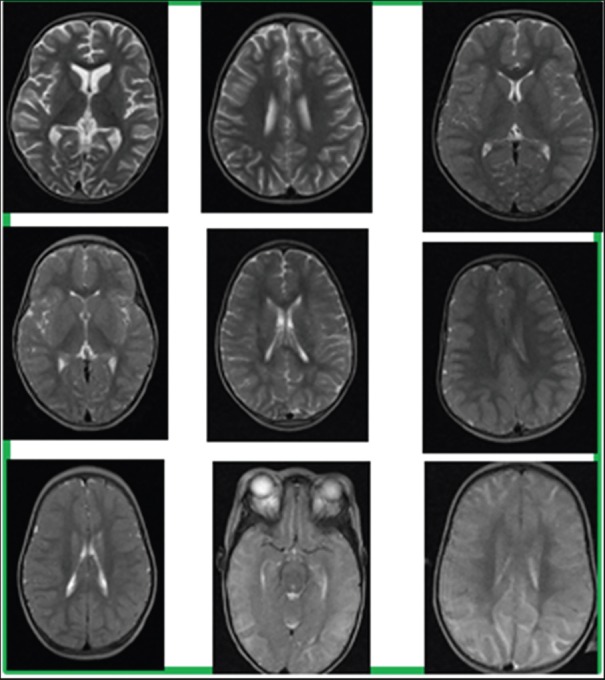
Increased brain volume (BV) and subsequent herniation are strongly associated with death in pediatric cerebral malaria (PCM), a leading killer of children in developing countries. Accurate noninvasive measures of BV are needed for optimal clinical trial design. Our objectives were to examine the performance of six different magnetic resonance imaging (MRI) BV quantification measures for predicting mortality in PCM and to review the advantages and disadvantages of each method.
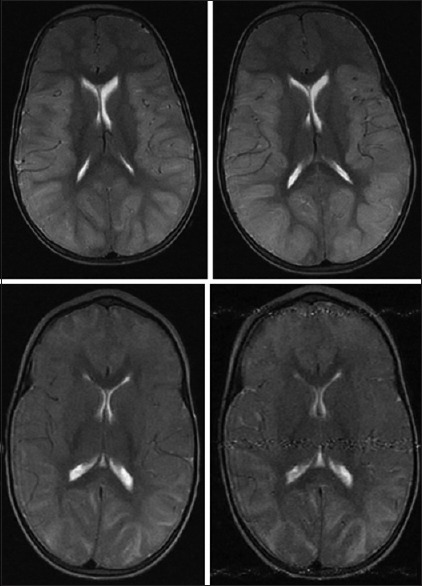
Receiver operator characteristics were generated from BV measures of MRIs of children admitted to an ongoing research project with PCM between 2009 and 2014. Fatal cases were matched to the next available survivor. A total of 78 MRIs of children aged 5 months to 13 years (mean 4.0 years), of which 45% were males, were included.
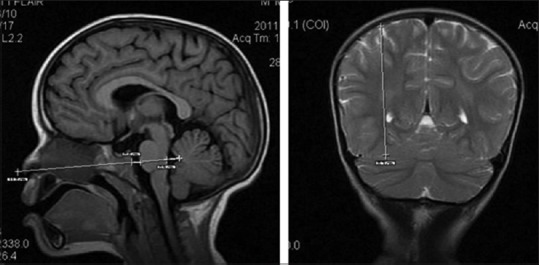
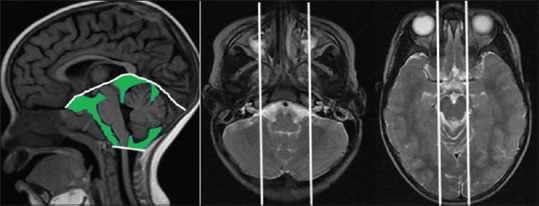
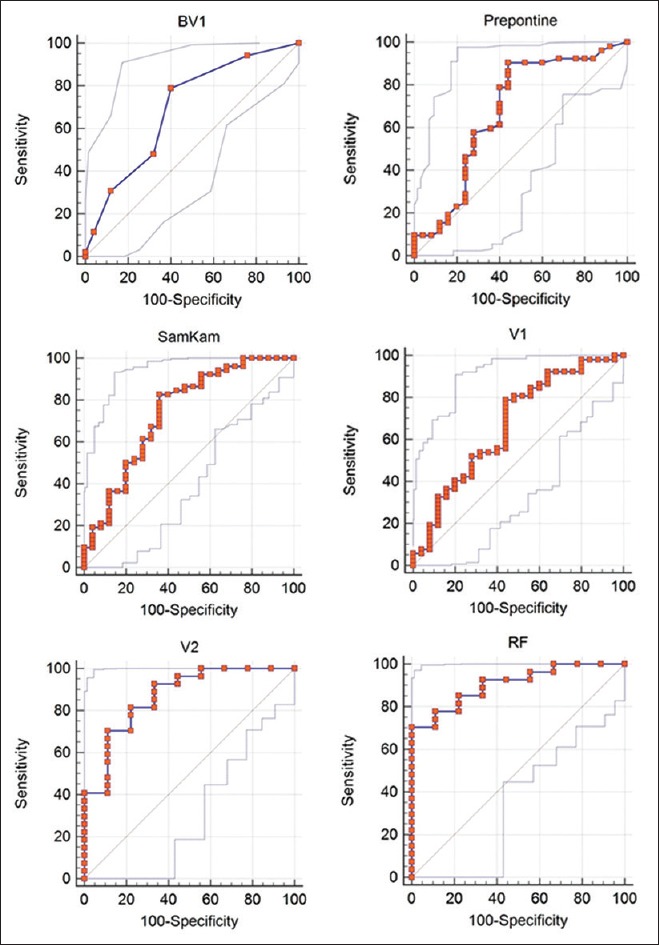
Areas under the curve (AUC) with 95% confidence interval on measures from the initial MRIs were: Radiologist-derived score = 0.69 (0.58-0.79; = 0.0037); prepontine cistern anteroposterior (AP) dimension = 0.70 (0.56-0.78; = 0.0133); SamKam ratio [Rt. parietal lobe height/(prepontine AP dimension + fourth ventricle AP dimension)] = 0.74 (0.63-0.83; = 0.0002); and global cerebrospinal fluid (CSF) space ascertained by ClearCanvas = 0.67 (0.55-0.77; = 0.0137). For patients with serial MRIs ( = 37), the day 2 global CSF space AUC was 0.87 (0.71-0.96; < 0.001) and the recovery factor (CSF volume day 2/CSF volume day 1) was 0.91 (0.76-0.98; < 0.0001). Poor prognosis is associated with radiologist score of ≥7; prepontine cistern dimension ≤3 mm; cisternal CSF volume ≤7.5 ml; SamKam ratio ≥6.5; and recovery factor ≤0.75.
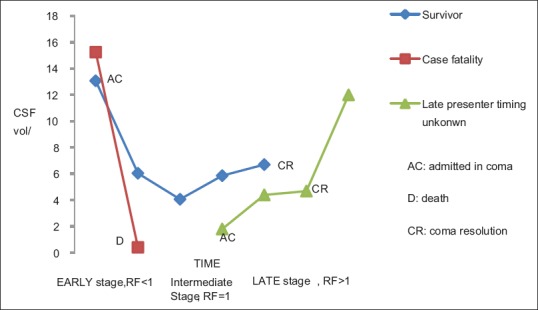
All noninvasive measures of BV performed well in predicting death and providing a proxy measure for brain volume. Initial MRI assessment may inform future clinical trials for subject selection, risk adjustment, or stratification. Measures of temporal change may be used to stage PCM.
脑容量(BV)增加及随后的脑疝与儿童脑型疟疾(PCM)的死亡密切相关,PCM是发展中国家儿童的主要杀手。为了优化临床试验设计,需要准确的无创性脑容量测量方法。我们的目标是检验六种不同的磁共振成像(MRI)脑容量量化测量方法在预测PCM死亡率方面的性能,并综述每种方法的优缺点。
从2009年至2014年参与一项正在进行的PCM研究项目的儿童MRI的脑容量测量数据中生成受试者工作特征曲线。将死亡病例与下一个可用的幸存者进行匹配。共纳入78例年龄在5个月至13岁(平均4.0岁)的儿童的MRI,其中45%为男性。
初始MRI测量指标的曲线下面积(AUC)及其95%置信区间为:放射科医生得出的评分=0.69(0.58 - 0.79;P = 0.0037);脑桥前池前后径(AP)=0.70(0.56 - 0.78;P = 0.0133);SamKam比率[右顶叶高度/(脑桥前AP径+第四脑室AP径)]=0.74(0.63 - 0.83;P = 0.0002);以及通过ClearCanvas确定的全脑脊髓液(CSF)间隙=0.67(0.55 - 0.77;P = 0.0137)。对于有系列MRI检查的患者(n = 37),第2天全脑CSF间隙的AUC为0.87(0.71 - 0.96;P < 0.001),恢复因子(第2天CSF体积/第1天CSF体积)为0.91(0.76 - 0.98;P < 0.0001)。预后不良与以下情况相关:放射科医生评分≥7;脑桥前池径≤3mm;脑池CSF体积≤7.5ml;SamKam比率≥6.5;以及恢复因子≤0.75。
所有无创性脑容量测量方法在预测死亡和提供脑容量替代测量方面表现良好。初始MRI评估可为未来临床试验的受试者选择、风险调整或分层提供参考。时间变化测量可用于对PCM进行分期。