Agency for Care Effectiveness, Ministry of Health, Harrower Hall, 14 College Road, Singapore, 169853, Singapore.
Division of Medical Oncology, National Cancer Centre Singapore, 11 Hospital Drive, Singapore, 169610, Singapore.
BMC Cancer. 2018 Mar 27;18(1):352. doi: 10.1186/s12885-018-4223-y.
Non-small-cell lung cancer (NSCLC) accounts for 85% of all lung cancers and is associated with a poor prognosis. Afatinib is an irreversible ErbB family blocker recommended in clinical guidelines as a first-line treatment for NSCLC which harbours an epidermal growth factor receptor (EGFR) mutation. The objective of this study was to evaluate the cost-effectiveness of afatinib versus pemetrexed-cisplatin for first-line treatment of locally advanced or metastatic EGFR mutation positive NSCLC in Singapore.
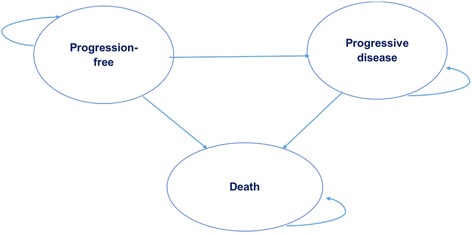
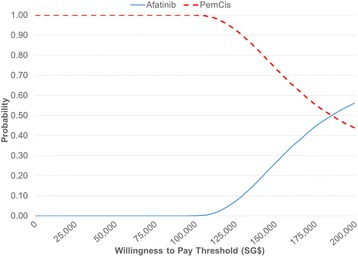
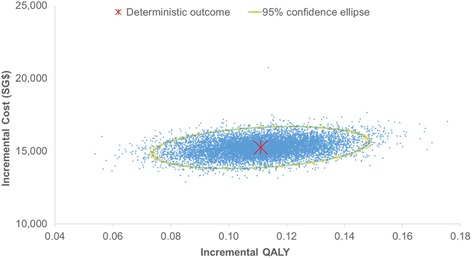
A partitioned survival model with three health states (progression-free, progressive disease and death) was developed from a healthcare payer perspective. Survival curves from the LUX-Lung 3 trial (afatinib versus pemetrexed-cisplatin chemotherapy) were extrapolated beyond the trial period to estimate the underlying progression-free survival and overall survival parametric distributions. Rates of adverse reactions were also estimated from LUX-Lung 3 while health utilities from overseas were derived from the literature in the absence of local estimates. Direct costs were sourced from public healthcare institutions in Singapore. Incremental cost-effectiveness ratios (ICERs) were calculated over a 5 year time horizon. Deterministic and probabilistic sensitivity analyses and additional scenario analyses were conducted to explore the impact of uncertainties and assumptions on the cost-effectiveness results.
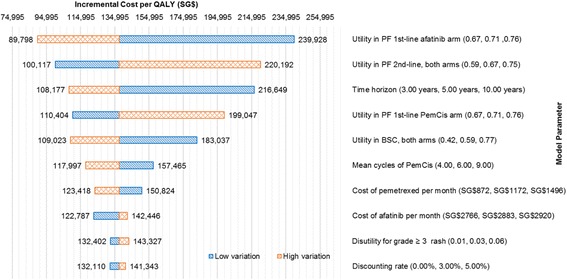
In the base-case analysis, the ICER for afatinib versus pemetrexed-cisplatin was SG$137,648 per quality-adjusted life year (QALY) gained and SG$109,172 per life-year gained. One-way sensitivity analysis showed the ICER was most sensitive to variations in the utility values, the cost of afatinib and time horizon. Scenario analyses showed that even reducing the cost of afatinib by 50% led to a high ICER which was unlikely to represent a cost-effective use of healthcare resources.
Compared with pemetrexed-cisplatin, afatinib is not cost-effective as a first-line treatment for advanced EGFR mutation-positive NSCLC in Singapore. The findings from our study will be useful to inform local healthcare decision-making and resource allocations for NSCLC treatments, together with other considerations such as clinical effectiveness, safety and affordability of TKIs.
非小细胞肺癌(NSCLC)占所有肺癌的 85%,预后较差。阿法替尼是一种不可逆的 ErbB 家族阻滞剂,被临床指南推荐为 EGFR 突变的 NSCLC 的一线治疗药物。本研究旨在评估阿法替尼与培美曲塞-顺铂相比,在治疗新加坡局部晚期或转移性 EGFR 突变阳性 NSCLC 中的成本效益。
从医疗保健支付者的角度出发,建立了一个具有三个健康状态(无进展、疾病进展和死亡)的分割生存模型。从 LUX-Lung 3 试验(阿法替尼与培美曲塞-顺铂化疗)中推断出生存曲线,以估计无进展生存和总生存的潜在参数分布。从 LUX-Lung 3 试验中估计不良反应的发生率,而健康效用则从海外文献中得出,因为缺乏当地估计值。直接成本来自新加坡的公共医疗机构。在 5 年的时间内计算增量成本效益比(ICER)。进行确定性和概率敏感性分析以及其他情景分析,以探讨不确定性和假设对成本效益结果的影响。
在基础案例分析中,阿法替尼与培美曲塞-顺铂相比的 ICER 为每获得 1 个质量调整生命年(QALY)需支付 137,648 新加坡元,每获得 1 个生命年需支付 109,172 新加坡元。单因素敏感性分析表明,ICER 对效用值、阿法替尼的成本和时间范围的变化最为敏感。情景分析表明,即使将阿法替尼的成本降低 50%,也会导致 ICER 非常高,这不太可能代表对医疗资源的有效利用。
与培美曲塞-顺铂相比,阿法替尼作为新加坡晚期 EGFR 突变阳性 NSCLC 的一线治疗药物并不具有成本效益。本研究的结果将有助于为 NSCLC 治疗的本地医疗保健决策和资源分配提供信息,同时还需要考虑其他因素,如临床效果、安全性和 TKI 的可负担性。