Fang Dong, He Shiming, Xiong Gengyan, Singla Nirmish, Cao Zhenpeng, Zhang Lei, Li Xuesong, Zhou Liqun
Department of Urology, Peking University First Hospital, Institute of Urology, Peking University, National Urological Cancer Centre, No. 8 Xishiku St, Xicheng District, Beijing, 100034, China.
Department of Urology, University of Texas Southwestern Medical Center, Dallas, TX, USA.
BMC Urol. 2018 Mar 27;18(1):22. doi: 10.1186/s12894-018-0334-7.
There's no consensus about the difference between renal pelvic and ureteral tumors in terms of clinical features, pathological outcomes, epigenetic biomarkers and prognosis.
The data of 341 patients with renal pelvic tumors and 271 patients with ureteral tumors who underwent radical nephroureterectomy between 1999 and 2011 were retrospectively reviewed. The clinicopathologic features, gene promoters methylation status and oncologic outcomes were compared. Regression analysis was performed to identify oncologic prognosticators.
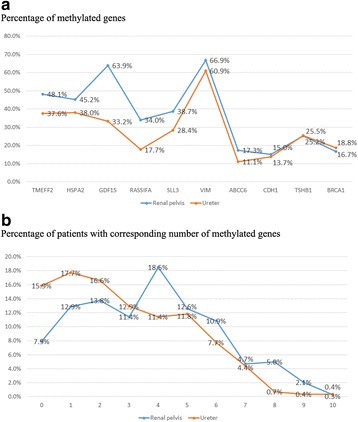
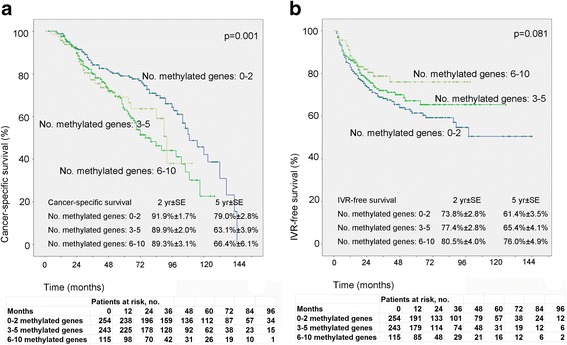
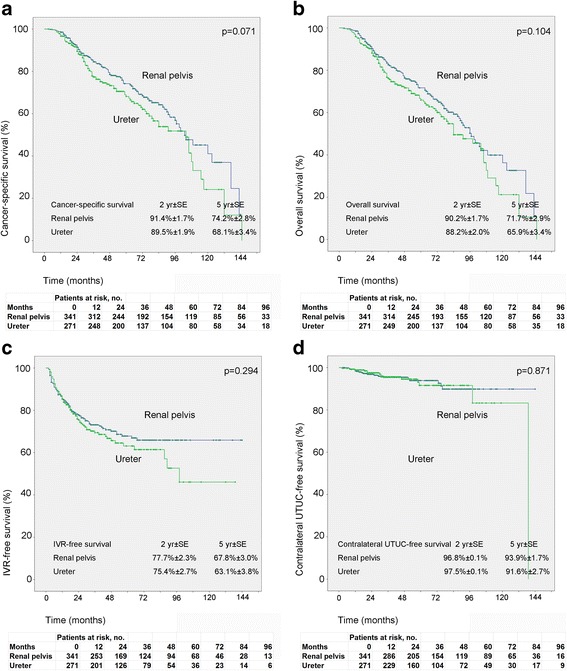
Patients with ureteral tumors were relatively older (p = 0.002), and had higher likelihood of pre-operative renal insufficiency (p < 0.001), hypertension (p = 0.038) and hydronephrosis (P < 0.001), while in patients with renal pelvic tumors gross hematuria was more prevalent (p < 0.001). Renal pelvic tumors tended to exhibit non-organ-confined disease (p = 0.004) and larger tumor diameter (p = 0.001), while ureteral tumors had a higher likelihood of exhibiting high grade (p < 0.001) and sessile architecture (p = 0.023). Hypermethylated gene promoters were significantly more prevalent in renal pelvic tumors (p < 0.001), specifically for TMEFF2, GDF15, RASSF1A, SALL3 and ABCC6 (all p < 0.05). Tumor location failed to independently predict cancer-specific survival, overall survival, intravesical or contralateral recurrence (all p > 0.05), while gene methylation status was demonstrated to be an independent prognostic factor.
Renal pelvic tumors and ureteral tumors exhibited significant differences in clinicopathologic characteristics and epigenetic biomarkers. Gene promoter methylation might be an important mechanism in explaining distinct tumor patterns and behaviors in UTUC.
肾盂肿瘤和输尿管肿瘤在临床特征、病理结果、表观遗传生物标志物及预后方面的差异尚无定论。
回顾性分析1999年至2011年间接受根治性肾输尿管切除术的341例肾盂肿瘤患者和271例输尿管肿瘤患者的数据。比较其临床病理特征、基因启动子甲基化状态及肿瘤学结局。进行回归分析以确定肿瘤学预后因素。
输尿管肿瘤患者年龄相对较大(p = 0.002),术前肾功能不全(p < 0.001)、高血压(p = 0.038)及肾积水(p < 0.001)的可能性更高,而肾盂肿瘤患者肉眼血尿更为常见(p < 0.001)。肾盂肿瘤倾向于表现为非器官局限性疾病(p = 0.004)且肿瘤直径较大(p = 0.001),而输尿管肿瘤表现为高级别(p < 0.001)及无蒂结构(p = 0.023)的可能性更高。高甲基化基因启动子在肾盂肿瘤中显著更为常见(p < 0.001),特别是TMEFF2、GDF15、RASSF1A、SALL3和ABCC6(均p < 0.05)。肿瘤位置不能独立预测癌症特异性生存、总生存、膀胱内或对侧复发(均p > 0.05),而基因甲基化状态被证明是一个独立的预后因素。
肾盂肿瘤和输尿管肿瘤在临床病理特征和表观遗传生物标志物方面存在显著差异。基因启动子甲基化可能是解释上尿路尿路上皮癌不同肿瘤模式和行为的重要机制。