Division of Vascular Surgery, Department of Surgery, Stanford University, Stanford, Calif; Surgical Services, VA Palo Alto Medical Center, Palo Alto, Calif.
Division of Vascular Surgery and Endovascular Therapy, Department of Surgery, Emory University School of Medicine, Atlanta, Ga.
J Vasc Surg. 2018 Aug;68(2):536-545.e2. doi: 10.1016/j.jvs.2017.10.092. Epub 2018 Mar 24.
Peripheral artery disease (PAD) is an increasing health concern with rising incidence globally. Previous studies have shown an association between PAD incidence and depression. The objective of the study was to determine the association of comorbid depression with PAD outcomes (amputation and all-cause mortality rates) in veterans.
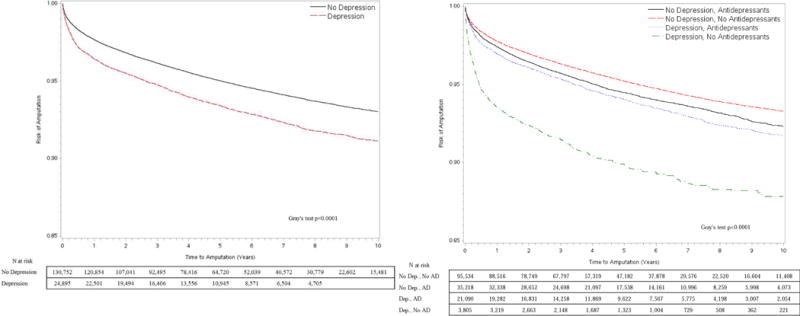
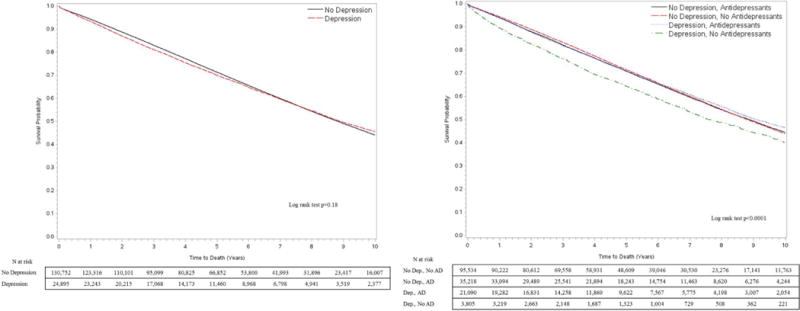
An observational retrospective cohort of 155,647 patients with incident PAD (2003-2014) from nationwide U.S. Veterans Health Administration hospitals was conducted using the national Veterans Affairs Corporate Data Warehouse. Depression was measured using concurrent International Classification of Diseases, Ninth Revision diagnosis codes 6 months before or after PAD diagnosis. The main outcomes were incident major amputation and all-cause mortality. Crude associations were assessed with Kaplan-Meier plots. The effects of depression adjusted for covariates were analyzed using Cox proportional hazards models.
Depression was present in 16% of the cohort, with the occurrence of 9517 amputations and 63,287 deaths (median follow-up, 5.9 years). Unadjusted hazard ratios (HRs) of comorbid depression for amputations and all-cause mortality were 1.32 (95% confidence interval [CI], 1.25-1.39) and 1.02 (95% CI, 0.99-1.04), respectively. After adjustment for covariates in Cox regression models, a diagnosis of comorbid depression at the time of PAD diagnosis was associated with a 13% higher amputation (HR, 1.13; 95% CI, 1.07-1.19) and 17% higher mortality (HR, 1.17; 95% CI, 1.14-1.20) risk compared with patients with no depression. On stratification by use of antidepressants, depressed patients not taking antidepressants had a 42% higher risk of amputation (HR, 1.42; 95% CI, 1.27-1.58) compared with those without depression. Patients taking antidepressants for depression still had increased risk of amputation but only 10% higher compared with those without depression (HR, 1.10; 95% CI, 1.03-1.17). Interestingly, patients taking antidepressants for other indications also had a higher risk of amputation compared with those not having depression or not taking antidepressants (HR, 1.08; 95% CI, 1.03-1.14). Having any diagnosis of depression or the need for antidepressants increased the mortality risk by 18% to 25% in the PAD cohort compared with those without depression and not taking antidepressants for any other indication.
PAD patients with comorbid depression have a significantly higher risk of amputation and mortality than PAD patients without depression. Furthermore, untreated depression was associated with an increased amputation risk in the PAD population, more so than depression or other mental illness being treated by antidepressants. The underlying mechanisms for causality, if any, remain to be determined. The association of antidepressant treatment use with amputation risk should prompt further investigations into possible mechanistic links between untreated depression and vascular dysfunction.
外周动脉疾病(PAD)是一种日益严重的健康问题,在全球范围内发病率不断上升。先前的研究表明,PAD 的发病率与抑郁症之间存在关联。本研究的目的是确定合并抑郁症与退伍军人 PAD 结局(截肢率和全因死亡率)之间的关系。
使用全国退伍军人事务部公司数据仓库,对 2003 年至 2014 年期间全国美国退伍军人健康管理局医院的 155647 例 PAD 新发病例进行了一项观察性回顾性队列研究。使用同期国际疾病分类,第 9 版诊断代码在 PAD 诊断前或后 6 个月内测量抑郁症。主要结局为新发主要截肢和全因死亡率。使用 Kaplan-Meier 图评估粗关联。使用 Cox 比例风险模型分析调整协变量后抑郁的影响。
队列中有 16%的患者合并抑郁症,发生了 9517 例截肢和 63287 例死亡(中位随访时间为 5.9 年)。未调整的合并抑郁症的截肢和全因死亡率的风险比(HR)分别为 1.32(95%置信区间[CI],1.25-1.39)和 1.02(95%CI,0.99-1.04)。在 Cox 回归模型中调整协变量后,PAD 诊断时合并抑郁症的诊断与 13%的更高截肢风险(HR,1.13;95%CI,1.07-1.19)和 17%的更高死亡率风险(HR,1.17;95%CI,1.14-1.20)相关与无抑郁症的患者相比。按使用抗抑郁药分层,未服用抗抑郁药的抑郁症患者截肢风险增加 42%(HR,1.42;95%CI,1.27-1.58)与无抑郁症的患者相比。服用抗抑郁药治疗抑郁症的患者仍有更高的截肢风险,但仅比无抑郁症的患者高 10%(HR,1.10;95%CI,1.03-1.17)。有趣的是,服用抗抑郁药治疗其他适应症的患者与未患有抑郁症或未服用抗抑郁药治疗其他任何适应症的患者相比,截肢风险也更高(HR,1.08;95%CI,1.03-1.14)。与未患有抑郁症且未因任何其他原因服用抗抑郁药的患者相比,在 PAD 队列中,任何抑郁症或抗抑郁药治疗的需求都使死亡率风险增加 18%至 25%。
与无抑郁症的 PAD 患者相比,合并抑郁症的 PAD 患者的截肢和死亡率风险显著更高。此外,未经治疗的抑郁症与 PAD 人群的截肢风险增加有关,比使用抗抑郁药治疗抑郁症或其他精神疾病更为明显。如果存在因果关系的机制,仍有待确定。抗抑郁药治疗与截肢风险之间的关联应促使进一步调查未治疗抑郁症与血管功能障碍之间可能存在的机制联系。