Wheat Joseph, Myint Thein, Guo Ying, Kemmer Phebe, Hage Chadi, Terry Colin, Azar Marwan M, Riddell James, Ender Peter, Chen Sharon, Shehab Kareem, Cleveland Kerry, Esguerra Eden, Johnson James, Wright Patty, Douglas Vanja, Vergidis Pascalis, Ooi Winnie, Baddley John, Bamberger David, Khairy Raed, Vikram Holenarasipur R, Jenny-Avital Elizabeth, Sivasubramanian Geetha, Bowlware Karen, Pahud Barbara, Sarria Juan, Tsai Townson, Assi Maha, Mocherla Satish, Prakash Vidhya, Allen David, Passaretti Catherine, Huprikar Shirish, Anderson Albert
Mira Vista Diagnostics University of Kentucky School of Medicine, Lexington, Kentucky Emory University Rollins School of Public Health Indiana University School of Medicine Indiana University Health, Indianapolis, Indiana Yale University School of Medicine, New Haven, Connecticut University of Michigan Health System, Ann Arbor, Michigan St. Luke's University Hospital and Health Network, Bethlehem Stanford University School of Medicine, Stanford University of Arizona College of Medicine, Tucson University of Tennessee Health Sciences Center, Memphis Mercy Hospital, Joplin Vanderbilt University School of Medicine, Nashville, Tennessee University of California at San Francisco School of Medicine, San Francisco University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania Lahey Hospital and Medical Center, Burlington, Massachusetts University of Alabama- Birmingham, Birmingham, Alabama University of Missouri-Kansas City, Kansas City Sparks Center for Infectious Diseases, Fort Smith, Arkansas Mayo Clinic, Phoenix, Arizona Jacobi Medical Center, Bronx Metro Infectious Diseases, Chicago University of Oklahoma Health Sciences Center, Oklahoma City, Oklahoma Children's Mercy Hospital, Kansas City, Missouri University of Texas Medical Branch, Galveston Kaiser Permanente, Los Angeles, California Infectious Disease Consultants, Wichita, Kansas Premier Physicians, Midland, Texas Southern Illinois University School of Medicine, Springfield, Illinois Courage Fund, National University of Singapore, Singapore Carolinas Medical Center, Charlotte, North Carolina Icahn School of Medicine at Mount Sinai, New York, New York Emory University School of Medicine, Atlanta, Georgia.
Medicine (Baltimore). 2018 Mar;97(13):e0245. doi: 10.1097/MD.0000000000010245.
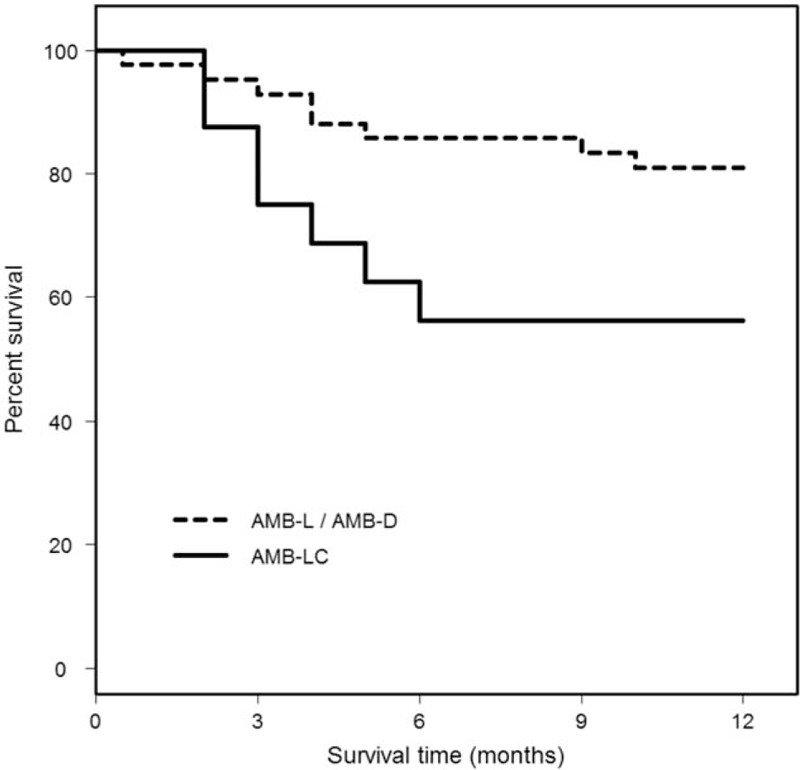
Central nervous system (CNS) involvement occurs in 5 to 10% of individuals with disseminated histoplasmosis. Most experience has been derived from small single center case series, or case report literature reviews. Therefore, a larger study of central nervous system (CNS) histoplasmosis is needed in order to guide the approach to diagnosis, and treatment.A convenience sample of 77 patients with histoplasmosis infection of the CNS was evaluated. Data was collected that focused on recognition of infection, diagnostic techniques, and outcomes of treatment.Twenty nine percent of patients were not immunosuppressed. Histoplasma antigen, or anti-Histoplasma antibodies were detected in the cerebrospinal fluid (CSF) in 75% of patients. One year survival was 75% among patients treated initially with amphotericin B, and was highest with liposomal, or deoxycholate formulations. Mortality was higher in immunocompromised patients, and patients 54 years of age, or older. Six percent of patients relapsed, all of whom had the acquired immunodeficiency syndrome (AIDS), and were poorly adherent with treatment.While CNS histoplasmosis occurred most often in immunocompromised individuals, a significant proportion of patients were previously, healthy. The diagnosis can be established by antigen, and antibody testing of the CSF, and serum, and antigen testing of the urine in most patients. Treatment with liposomal amphotericin B (AMB-L) for at least 1 month; followed by itraconazole for at least 1 year, results in survival among the majority of individuals. Patients should be followed for relapse for at least 1 year, after stopping therapy.
5%至10%播散性组织胞浆菌病患者会出现中枢神经系统(CNS)受累。大多数经验来自小型单中心病例系列研究或病例报告文献综述。因此,需要开展更大规模的中枢神经系统(CNS)组织胞浆菌病研究,以指导诊断和治疗方法。
对77例中枢神经系统组织胞浆菌病感染患者的便利样本进行了评估。收集了侧重于感染识别、诊断技术和治疗结果的数据。
29%的患者没有免疫抑制。75%的患者脑脊液(CSF)中检测到组织胞浆菌抗原或抗组织胞浆菌抗体。最初接受两性霉素B治疗的患者一年生存率为75%,脂质体或脱氧胆酸盐制剂的生存率最高。免疫功能低下患者以及54岁及以上患者的死亡率更高。6%的患者复发,所有复发患者均患有获得性免疫缺陷综合征(AIDS),且治疗依从性差。
虽然中枢神经系统组织胞浆菌病最常发生在免疫功能低下的个体中,但相当一部分患者以前是健康的。大多数患者可通过脑脊液和血清的抗原及抗体检测以及尿液抗原检测来确诊。用脂质体两性霉素B(AMB-L)治疗至少1个月;随后用伊曲康唑治疗至少1年,大多数患者可存活。停药后应随访患者至少1年,观察是否复发。