Øra Hege Prag, Kirmess Melanie, Brady Marian C, Winsnes Ingvild Elisabeth, Hansen Silje Merethe, Becker Frank
Sunnaas Rehabilitation Hospital, Bjørnemyrveien 11, 1450, Nesoddtangen, Norway.
Institute of Clinical Medicine, University of Oslo, PO Box 1171, Blindern, 0318, Oslo, Norway.
Trials. 2018 Apr 2;19(1):208. doi: 10.1186/s13063-018-2588-5.
The Cochrane review on the effectiveness of speech and language therapy for aphasia following stroke suggests intensity of therapy is a key predictor for outcome. Current aphasia services cannot provide intervention at the intensity observed within trial contexts because of resource limitations. Telerehabilitation could widen access to speech-language pathologists (SLPs) in geographically remote contexts and reduce the time spent on travel by the therapist and patient. The current academic literature within this field is in its infancy, with few trials of speech and language therapy (SLT) delivered by videoconference. Our pilot randomized controlled trial (RCT) will explore feasibility aspects and effectiveness of telerehabilitation for aphasia in addition to standard SLT.
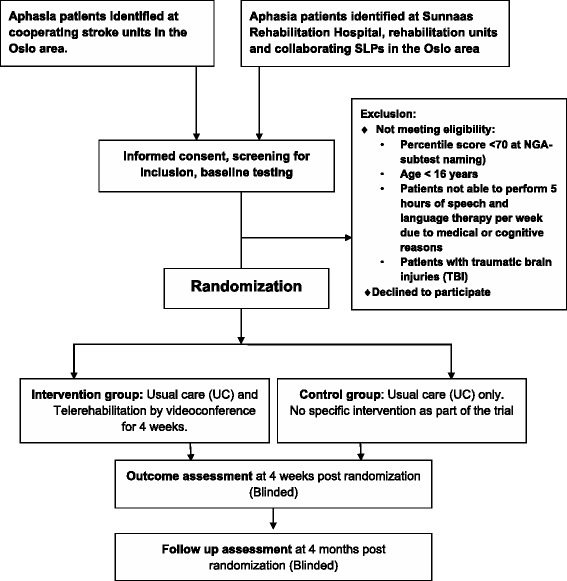
METHOD/DESIGN: Our study is a pragmatic, exploratory, pilot randomized controlled trial, where participants will be randomized to a telerehabilitation group or a control group. Both groups receive standard SLT (usual care) but the telerehabilitation group receives an additional 5 h of telerehabilitation per week over 4 weeks through videoconference. This additional telerehabilitation focuses on spoken language with an emphasis on word naming. We aim to include 40 patients in each group, with inclusion criteria being aphasia any time post stroke. Participants will be assessed blindly at pre-randomization (baseline), and 4 weeks and 4 months after randomization. The primary endpoint is naming ability 3 months after the completed intervention, measured by the Norwegian Basic Aphasia Assessment (NGA) naming subtest. Secondary endpoints include other subtests of the NGA, the VAST (Verb and Sentence Test) subtest sentence production, Communicative Effectiveness Index (CETI) and the Stroke and Aphasia Quality of Life scale (SAQOL-39). Experiences of patients and SLPs with telerehabilitation are assessed using questionnaires and semi-structured interviews. Statistical between group comparisons will be in line with an intention-to-treat analysis.
This pilot RCT of intensive language training by videoconference will contribute new scientific evidence to the field of aphasia telerehabilitation. Here, we describe our trial which will explore the feasibility of telerehabilitation for aphasia as an intervention, our choice of primary and secondary outcome measures and proposed analyses. Our trial will provide information for the development and delivery of future definitive RCTs.
ClinicalTrials.gov, ID: NCT02768922 . Registered on 11 May 2016. Last updated on 17 November 2017.
Cochrane关于中风后失语症言语和语言治疗有效性的综述表明,治疗强度是结果的关键预测因素。由于资源限制,目前的失语症服务无法在试验环境中观察到的强度下提供干预。远程康复可以扩大地理偏远地区获得言语治疗师(SLP)服务的机会,并减少治疗师和患者的出行时间。该领域目前的学术文献尚处于起步阶段,通过视频会议进行言语和语言治疗(SLT)的试验很少。我们的试点随机对照试验(RCT)除了标准的言语和语言治疗外,还将探索失语症远程康复的可行性和有效性。
方法/设计:我们的研究是一项务实、探索性的试点随机对照试验,参与者将被随机分配到远程康复组或对照组。两组均接受标准的言语和语言治疗(常规护理),但远程康复组在4周内每周通过视频会议额外接受5小时的远程康复治疗。这种额外的远程康复侧重于口语,重点是单词命名。我们的目标是每组纳入40名患者,纳入标准为中风后任何时间出现失语症。参与者将在随机分组前(基线)、随机分组后4周和4个月进行盲法评估。主要终点是完成干预3个月后的命名能力,通过挪威基本失语症评估(NGA)命名子测试进行测量。次要终点包括NGA的其他子测试、VAST(动词和句子测试)子测试句子生成、沟通有效性指数(CETI)和中风与失语症生活质量量表(SAQOL-39)。使用问卷和半结构化访谈评估患者和言语治疗师对远程康复的体验。组间统计比较将符合意向性分析。
这项通过视频会议进行强化语言训练的试点随机对照试验将为失语症远程康复领域提供新的科学证据。在此,我们描述了我们的试验,该试验将探索失语症远程康复作为一种干预措施的可行性、我们对主要和次要结局指标的选择以及拟议的分析方法。我们的试验将为未来确定性随机对照试验的开展和实施提供信息。
ClinicalTrials.gov,ID:NCT02768922。于2016年5月11日注册。最后更新于2017年11月17日。