Liu Guo, Ye Christine J, Chowdhury Saroj K, Abdallah Batoul Y, Horne Steven D, Nichols Denise, Heng Henry H
Center for Molecular Medicine and Genomics, Wayne State University School of Medicine, Detroit, MI48201, USA.
The Division of Hematology/Oncology, Department of Internal Medicine, University of Michigan, Ann Arbor, MI48109, USA.
Curr Genomics. 2018 Apr;19(3):200-206. doi: 10.2174/1389202918666170705150819.
Gulf War Illness (GWI) impacts 25-30% of gulf war veterans. Due to its heterogeneity in both etiology and symptoms, it has been challenging to establish the commonly accepted case definition for GWI. Equally challenging are the understanding of the general mechanism of GWI and the development of biomarkers useful for its clinical diagnosis and treatment.
We have observed that chromosome condensation defects can be detected in GWI patients. To document this phenomenon in GWI, we aim to describe and compare different types of chromosomal condensation defects in GWI patients, if possible. Since chromosomal condensation represents an important step of ensuring genome integrity, condensation defects could be used as a potential biomarker of GWI.
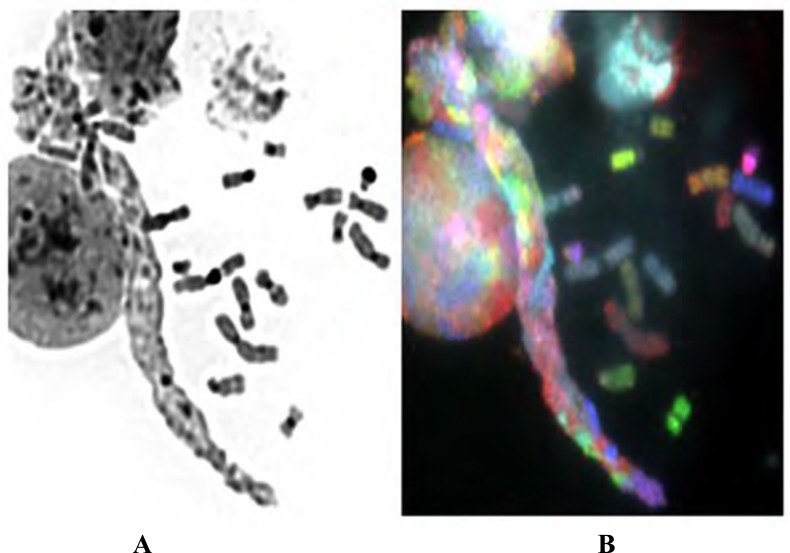
Lymphocytes from GWI patients have been used for short term cell culture followed by chromosome slide preparation. Both Giemsa staining and multiple color spectral karyotyping (SKY) were applied to study chromosome aberrations, focusing on different types of condensation defects.
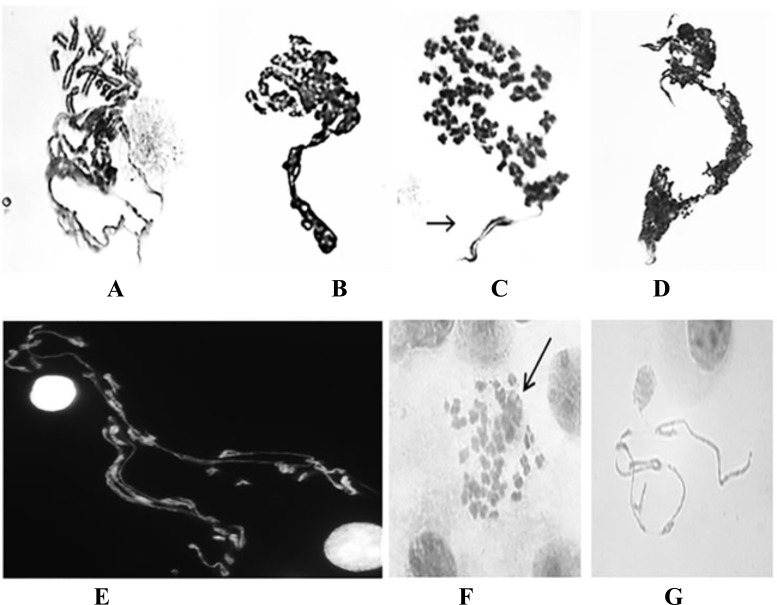
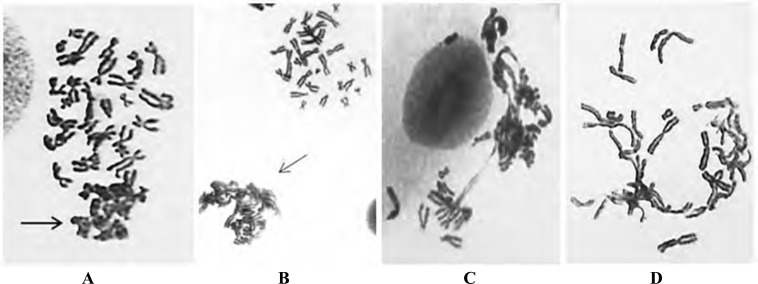
At least three subtypes of Defective Mitotic Figures (DMFs) were observed. Some individuals displayed elevated frequencies of DMFs. Another type of condensation defect identified as sticky chromosomes were also observed.
Various types of condensation defects have been observed in GWI patients. It is rather surprising that some GWI patients exhibited a high level of chromosomal condensation defects. Previously, the elevated frequency of DMFs was only observed in cancer patients. Since chromosome condensation can be linked to other types of chromosome aberrations, as well as cellular stress conditions, the detailed mechanism and clinical impact should be further studied, especially with increased sample size.
海湾战争综合征(GWI)影响着25%至30%的海湾战争退伍军人。由于其在病因和症状方面的异质性,为GWI建立普遍认可的病例定义一直具有挑战性。同样具有挑战性的是对GWI一般机制的理解以及开发用于其临床诊断和治疗的生物标志物。
我们观察到在GWI患者中可以检测到染色体凝聚缺陷。为了记录GWI中的这一现象,我们旨在尽可能描述和比较GWI患者中不同类型的染色体凝聚缺陷。由于染色体凝聚是确保基因组完整性的重要步骤,凝聚缺陷可作为GWI的潜在生物标志物。
使用GWI患者的淋巴细胞进行短期细胞培养,随后制备染色体玻片。吉姆萨染色和多色光谱核型分析(SKY)均用于研究染色体畸变,重点关注不同类型的凝聚缺陷。
观察到至少三种有缺陷的有丝分裂图像(DMF)亚型。一些个体显示出较高频率的DMF。还观察到另一种类型的凝聚缺陷,即粘性染色体。
在GWI患者中观察到了各种类型的凝聚缺陷。令人惊讶的是,一些GWI患者表现出高水平的染色体凝聚缺陷。以前,仅在癌症患者中观察到DMF频率升高。由于染色体凝聚可能与其他类型的染色体畸变以及细胞应激状况有关,因此应进一步研究其详细机制和临床影响,尤其是增加样本量之后。