School of Public Health and Community Medicine, the University of New South Wales, Sydney, Australia.
Department of Community Medicine, Women Medical and Dental College, Abbottabad, Pakistan.
BMC Public Health. 2018 Apr 2;18(1):428. doi: 10.1186/s12889-018-5363-3.
Reliable and timely data on maternal and neonatal mortality is required to implement health interventions, monitor progress, and evaluate health programs at national and sub-national levels. In most South Asian countries, including Pakistan, vital civil registration and health information systems are inadequate. The aim of this study is to determine accurate maternal and perinatal mortality through enhanced surveillance of births and deaths, compared with prior routinely collected data.
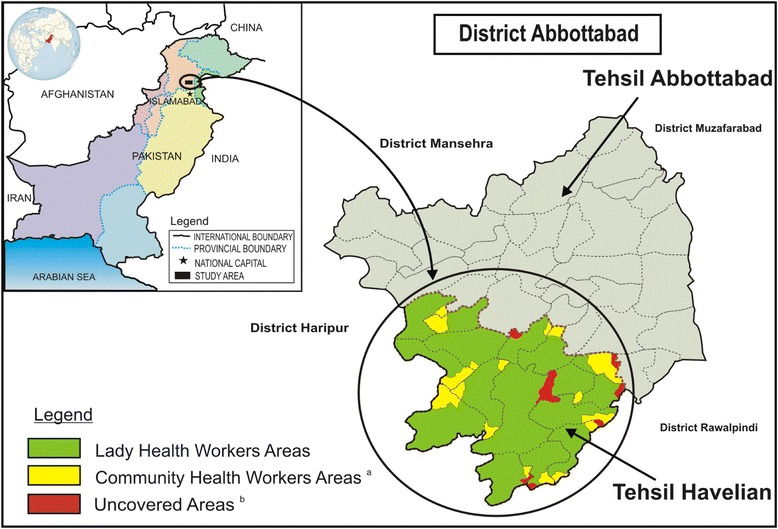
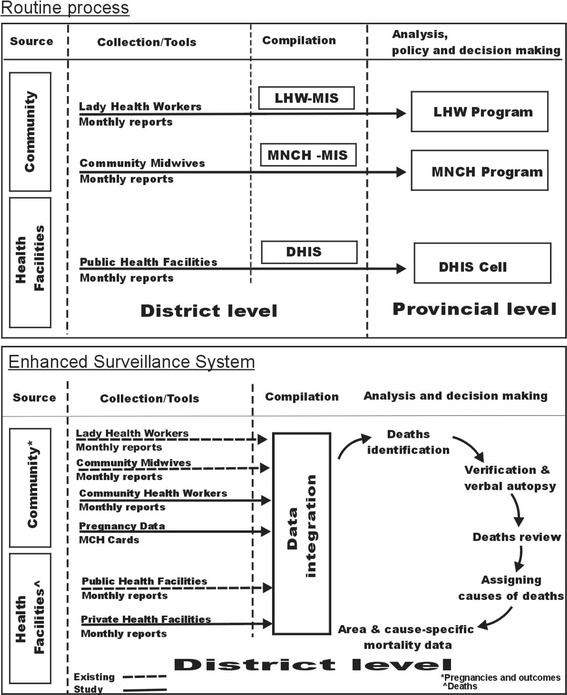
An enhanced surveillance system was established that measured maternal, perinatal and neonatal mortality rates through more complete enumeration of births and deaths in a rural district of Pakistan. Data were collected over a period of 1 year (2015/16) from augmentation of the existing health information system covering public healthcare facilities (n = 19), and the community through 273 existing Lady Health Workers; and with the addition of private healthcare facilities (n = 10), and 73 additional Community Health Workers to cover a total study population of 368,454 consisting of 51,690 eligible women aged 18 to 49 years with 7580 pregnancies and 7273 live births over 1 year. Maternal, neonatal, perinatal and stillbirth rates and ratios were calculated, with comparisons to routine reporting from the previous period (2014-15).
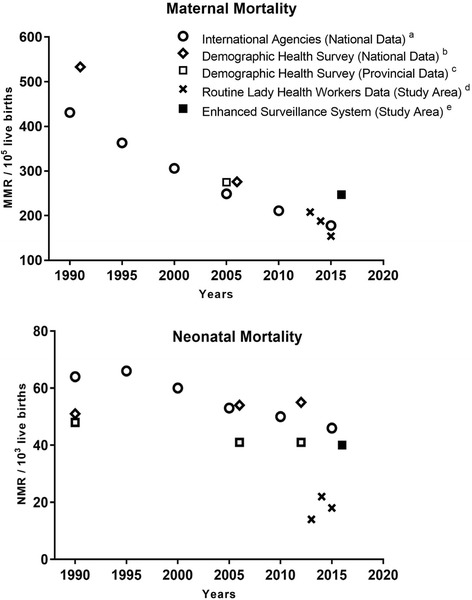
Higher maternal mortality, perinatal mortality and neonatal mortality rates were observed through enhanced surveillance compared to mortality rates in the previous 1.5 years from the routine monitoring system from increased completeness and coverage. Maternal mortality was 247 compared to 180 per 100, 000 live births (p = 0.36), neonatal mortality 40 compared to 20 per 1, 000 live births (p < 0.001), and perinatal mortality 60 compared to 47 per 1000 live births (p < 0.001). All the mortality rates were higher than provincial and national estimates proffered by international agencies based on successive Pakistan Demographic and Health Surveys and projections.
Extension of coverage and improvement in completeness through reconciliation of data from health information systems is possible and required to obtain accurate maternal, perinatal and neonatal mortality for assessment of health service interventions at a local level.
可靠且及时的孕产妇和新生儿死亡率数据对于在国家和次国家层面实施卫生干预措施、监测进展和评估卫生计划至关重要。在包括巴基斯坦在内的大多数南亚国家,基本的民事登记和卫生信息系统都不健全。本研究旨在通过更全面地统计出生和死亡人数,对分娩和死亡进行强化监测,从而确定更准确的孕产妇和围产期死亡率,与之前常规收集的数据进行比较。
建立了一个强化监测系统,通过更全面地统计巴基斯坦一个农村地区的出生和死亡人数,来测量孕产妇、围产期和新生儿死亡率。该系统在为期一年(2015/16 年)的数据收集期间,通过对现有卫生信息系统(覆盖公共医疗设施,n=19)和社区(通过 273 名现有女卫生工作者)的数据进行扩充,以及增加 10 家私营医疗设施和 73 名社区卫生工作者,对 368454 名研究人群(年龄在 18 至 49 岁之间的 51690 名合格妇女,7580 次妊娠和 7273 次活产)进行了调查。计算了孕产妇、新生儿、围产期和死产的死亡率和比例,并与前一时期(2014-15 年)的常规报告进行了比较。
与前一时期(2014-15 年)相比,通过强化监测,产妇死亡率、围产期死亡率和新生儿死亡率均有所上升,这是由于监测的完整性和覆盖面增加所致。与常规监测系统相比,强化监测系统下的产妇死亡率为每 10 万活产 247 例,而前一时期为每 10 万活产 180 例(p=0.36);新生儿死亡率为每 1000 例活产 40 例,而前一时期为每 1000 例活产 20 例(p<0.001);围产期死亡率为每 1000 例活产 60 例,而前一时期为每 1000 例活产 47 例(p<0.001)。所有这些死亡率都高于国际机构根据历届巴基斯坦人口与健康调查和预测提供的省级和国家估计数。
通过对卫生信息系统数据的协调,扩大覆盖范围和提高完整性是可能的,也是必要的,以便在地方一级评估卫生服务干预措施,获得准确的孕产妇、围产期和新生儿死亡率数据。