Lithgow Kirstie, Chin Alex, Debert Chantel T, Kline Gregory A
Division of Endocrinology, Department of Medicine, Cumming School of Medicine, University of Calgary, 1820 Richmond Rd SW, Calgary, AB, T2T 5C7, Canada.
Clinical Biochemistry, Calgary Laboratory Services and Department of Pathology and Laboratory Medicine, Cumming School of Medicine, University of Calgary, 9, 3535 Research Road NW, Calgary, AB, T2L 2K8, Canada.
BMC Endocr Disord. 2018 Apr 2;18(1):20. doi: 10.1186/s12902-018-0247-1.
Growth hormone deficiency (GHD) is a potential consequence of traumatic brain injury (TBI), including sport-related concussion (SRC). GH stimulation testing is required for definitive diagnosis; however, this is resource intensive and can be associated with adverse symptoms or risks. Measurement of serum IGF-1 is more practical and accessible, and pituitary tumour patients with hypopituitarism and low serum IGF-1 have been shown to have a high probability of GHD. We aimed to evaluate IGF-1 measurement for diagnosing GHD in our local TBI population.
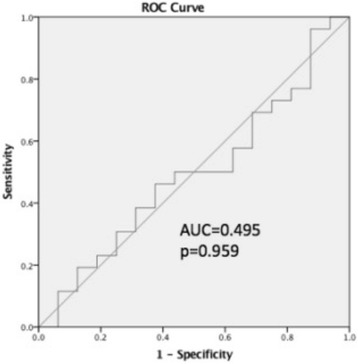
We conducted a retrospective chart review of patients evaluated for GHD at the TBI clinic and referred for GH stimulation testing with insulin tolerance test (ITT) or glucagon stimulation test (GST) since December 2013. We obtained demographics, TBI severity, IGF-1, data pertaining to pituitary function, and GH stimulation results. IGF-1 values were used to calculate z-scores per age and gender specific reference ranges. Receiver operator curve analysis was performed to evaluate diagnostic threshold of IGF-1 z-score for determining GHD by GST or ITT.
Sixty four patient charts were reviewed. 48 patients had mild, six had moderate, eight had severe TBI, and two had non-traumatic brain injuries. 47 patients underwent ITT or GST. 27 were confirmed to have GHD (peak hGH < 5 μg/L). IGF-1 level was within the age and gender specific reference range for all patients with confirmed GHD following GH stimulation testing. Only one patient had a baseline IGF-1 level below the age and gender specific reference range; this patient had a normal response to GH stimulation testing. ROC analysis showed IGF-1 z-score AUC f, confirming lack of diagnostic utility.
Baseline IGF-1 is not a useful predictor of GHD in our local TBI population, and therefore has no value as a screening tool. TBI patients undergoing pituitary evaluation will require a dynamic test of GH reserve.
生长激素缺乏症(GHD)是创伤性脑损伤(TBI)的潜在后果,包括与运动相关的脑震荡(SRC)。明确诊断需要进行生长激素刺激试验;然而,这需要大量资源,并且可能伴有不良症状或风险。血清胰岛素样生长因子-1(IGF-1)的测量更实用且更容易获得,并且垂体瘤伴垂体功能减退和低血清IGF-1的患者已被证明患GHD的可能性很高。我们旨在评估IGF-1测量在我们当地TBI人群中诊断GHD的价值。
我们对自2013年12月以来在TBI诊所接受GHD评估并被转诊进行胰岛素耐量试验(ITT)或胰高血糖素刺激试验(GST)的生长激素刺激试验的患者进行了回顾性病历审查。我们获取了人口统计学、TBI严重程度、IGF-1、与垂体功能相关的数据以及生长激素刺激结果。IGF-1值用于根据年龄和性别特异性参考范围计算z分数。进行受试者操作特征曲线分析以评估IGF-1 z分数对通过GST或ITT确定GHD的诊断阈值。
审查了64份患者病历。48例患者为轻度TBI,6例为中度,8例为重度,2例为非创伤性脑损伤。47例患者接受了ITT或GST。27例被确诊为GHD(生长激素峰值<5μg/L)。在生长激素刺激试验后,所有确诊为GHD的患者的IGF-1水平均在年龄和性别特异性参考范围内。只有1例患者的基线IGF-1水平低于年龄和性别特异性参考范围;该患者对生长激素刺激试验反应正常。ROC分析显示IGF-1 z分数曲线下面积,证实缺乏诊断效用。
在我们当地的TBI人群中,基线IGF-1不是GHD的有用预测指标,因此作为筛查工具没有价值。接受垂体评估的TBI患者需要进行生长激素储备的动态测试。